

Learn from babies
The dot tells you almost nothing. The line tells you everything.
Single observation
30th percentile. Healthy? Declining? You can’t tell.
Longitudinal view
80th → 30th. The line tells you everything.
The dot tells you almost nothing. The line tells you everything.
Imagine a visit to a paediatrician. They weigh the baby, measure the baby, and plot one dot on a chart. A baby steady on the 30th percentile is well. A baby who slides from the 80th to the 30th since the previous visit needs looking at immediately.
Dentistry has the same charts. We just don’t always draw the line.
N=1
We typically don’t make irreversible life decisions on a sample of one.
You wouldn’t sell your house for the first amount a stranger shouted over the fence. You wouldn’t amputate a leg because it ached on a Tuesday. We wait. We watch. We gather second, third and fourth data points, and crucially see where it’s trending, before we do something we can’t undo. We usually do this intuitively, subconsciously, and heuristically.
A lesion is not a thing, it’s a stage in a story, and the only honest question is which way the story of this lesion is heading. Understanding how quickly a condition is changing is often more informative than simply determining whether change has occurred.
Conditions that are a process
Sometimes it changes. Sometimes rapidly. Sometimes it stays still.
Signal or noise?
Single observations can be misleading. Longitudinal data separates true change from measurement noise.
Clinical measurements are never perfect. A radiograph may look different because of angulation. A periodontal measurement may vary between examinations. A lesion may appear larger or smaller because of lighting, photography, or examiner variability.
The clinician is rarely observing disease directly; they are observing a measurement of disease. Longitudinal monitoring helps separate true biological change from measurement noise, allowing the signal to emerge from the background variability.
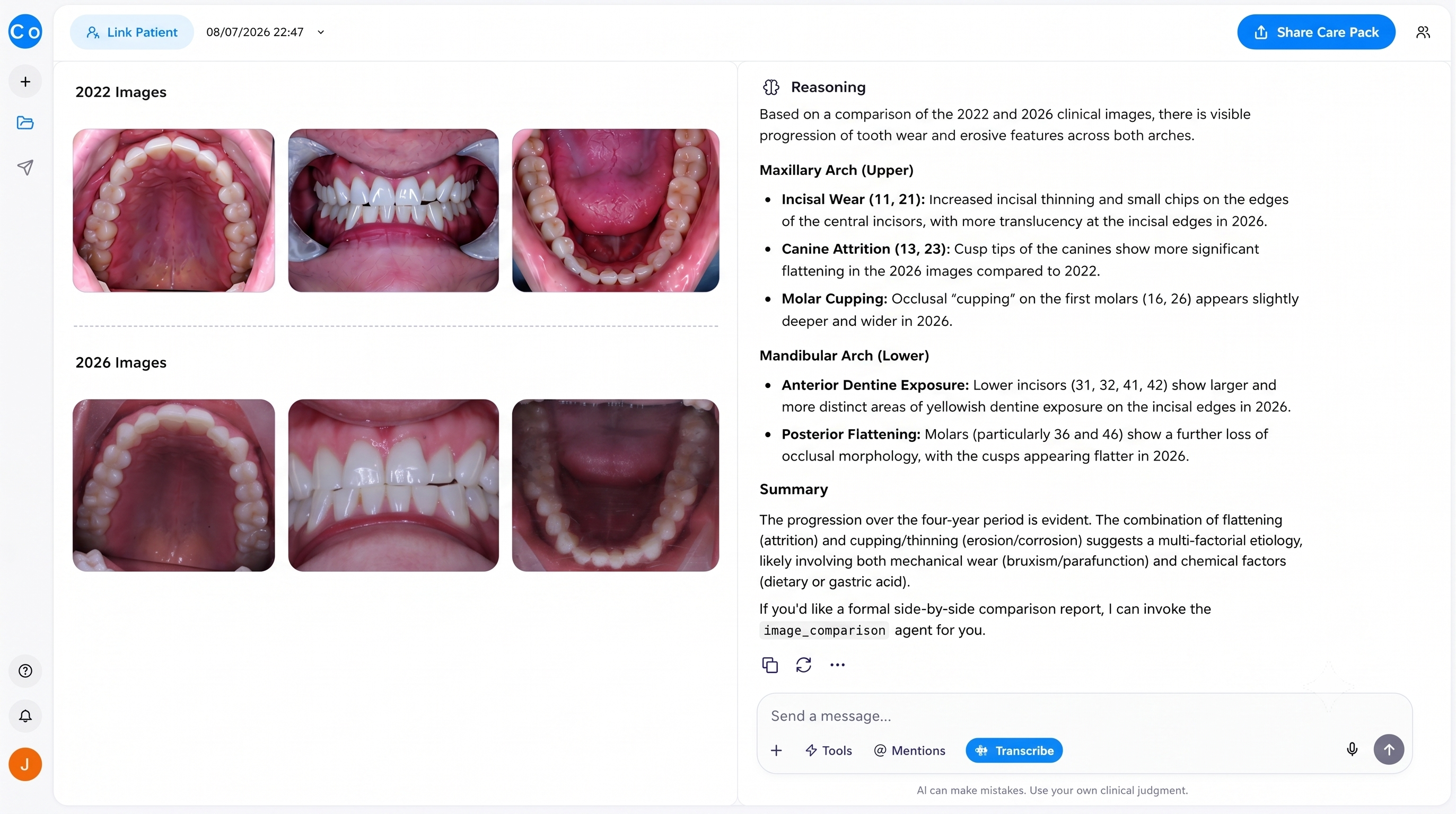
Four years apart, side by side. The AI reads the trend a single visit could never show.
Iatrogenesis from residual risk
Every irreversible intervention starts a second act you can’t control.
Not every lesion becomes disease. Not every disease becomes clinically significant. No one ever looked at a hurricane and blamed a butterfly. The chain is too long, the steps too many, the cause too far back to see. By the time a tooth needs an extraction at fifty, nobody remembers the fissure sealant at twenty one. We feel the hurricane. All we can do is minimise the wing beats where and when appropriate. Not every lesion becomes disease. Not every disease becomes clinically significant.
No intervention?
This is not an argument for doing nothing.
Watching can be its own harm. Some conditions are gathering storms, and the data says so. This is where experience, judgement and sound decision making make human practitioners indispensable.
Leave alone
- Condition is not moving
- Benefit does not outweigh residual risk
- Unlikely to progress to harm
Treat now
- Condition is trending toward bad outcome
- Earliest possible time to act
- Benefit clearly outweighs long-term risk
The aim is to treat the condition that is actually moving, at the earliest possible time when it starts moving and is trending towards a disastrous outcome.
Trust and persuasion
The data does the work. You take the measurement, plot the point, demonstrate the change.
Showing that a condition is stable, and that you’ll continue to monitor it, is one of the ways you build the most profound trust. Showing the condition is moving towards a very bad outcome, and being there with the options and solutions, is one of the easiest ways to earn case acceptance.
Stable condition
Patient trust built
Progressing condition
Case acceptance earned
The data moat
Your past data can be one of the strongest reasons a patient comes back to you.
“Come back in six months and we’ll see whether the wear is getting worse.”
Recall language that works
That sentence, if repeated, will improve your rebooking and recall attendance many fold. Remember though that this is conditional on regular gathering of photos, scans, and when indicated radiographs.
I’m a firm believer that if you treat your data as one of your most valuable assets, it will respond by becoming one of your most valuable assets.
Data value compounds over time
Ergodic nature
There’s a point where a condition no longer regresses to a mean, and pulls with increasing power towards a bad outcome.
Nassim Taleb calls ergodicity the most powerful concept he knows, and calls this exact point an absorbing barrier. Get close enough and there is no path back. A condition near that edge travels one way quickly toward full mouth rehab, clearance, or in the case of oral medicine, much worse outcomes.
Past a certain point, watching is not evidence based. It’s the road to an absorbing barrier and great harm. Doing nothing becomes a severely iatrogenic act.
In summary
Great patient and commercial outcomes should never be built on compromising ethics.
Longitudinal monitoring, with judicious data‑backed watch and wait strategies and judicious data‑backed intervention, is the best way to achieve excellent patient outcomes.
Gather longitudinal data
Photos, scans, and radiographs at every recall.
Watch what is stable
Monitoring a stable lesion is treatment. Name it as such.
Act on what is moving
The earliest point of trend is the optimal point of intervention.