Can a Root Canal Fail Years Later?
Yes, a tooth that had root canal treatment years ago can sometimes develop problems again if bacteria re-enter the canal system or the tooth structure weakens over time.



Short Answer
Yes, root canal treatment can occasionally fail months or even years later. Common reasons include reinfection, leakage around old restorations, missed canals, fractures, new decay, or persistent inflammation around the root.
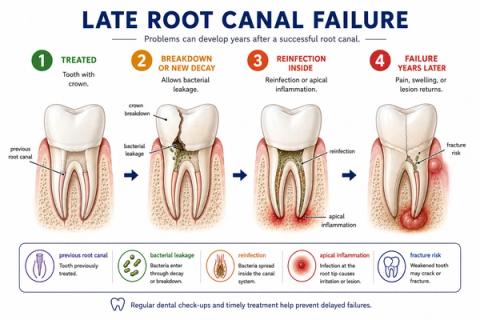
Why Can a Root Canal Fail Years Later?
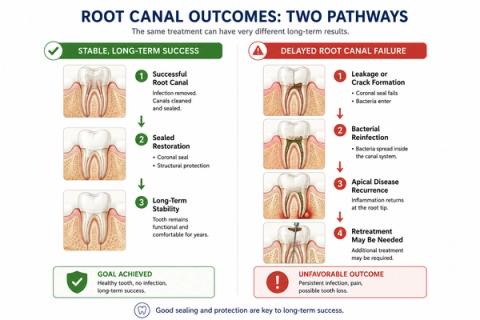
Root canal treatment can successfully preserve teeth for many years.
However:
- a treated tooth is still biologically and structurally vulnerable over time.
Problems may develop later if:
- bacteria re-enter the tooth,
- fillings or crowns leak,
- new decay forms,
- cracks develop,
- hidden canals were not fully cleaned initially,
- or inflammation around the root persists or returns.
Importantly:many root canal treated teeth remain stable long term,and:delayed failure does not automatically mean the original treatment was poorly performed.
What Symptoms Can Develop Years Later?
People may notice:
- renewed chewing or biting pain,
- swelling near the tooth,
- gum tenderness,
- pressure sensitivity,
- bad taste or drainage,
- recurring infection,
- or discomfort that slowly returns over time.
In some cases:
- changes may appear on X-rays before symptoms become obvious.
Some delayed failures remain:
- asymptomatic initially,while:
- apical inflammation progresses silently around the root.
Why Restoration Quality Matters Long Term
Long-term outcome depends on factors such as:
- restoration quality,
- structural integrity,
- bacterial control,
- crack formation,
- and overall oral health.
Even technically well-treated canals may later fail if:
- coronal leakage develops,
- restorations break down,
- recurrent decay occurs,
- or structural fatigue progresses over time.
This is why:
- long-term maintenance and restoration integrity remain critically important after root canal treatment.
Why the Pattern of Symptoms Matters
| Symptom Pattern | What It May Suggest |
|---|---|
| Mild stable function for years | Long-term successful adaptation |
| Renewed chewing or biting pain | Structural or apical reinvolvement |
| Swelling or drainage | Recurrent infection |
| Crown or filling loosening | Coronal leakage risk |
| Pressure sensitivity | Persistent apical inflammation |
| Localized biting pain | Possible crack or fracture |
| X-ray changes without symptoms | Silent apical recurrence |
- symptoms,
- radiographic healing,
- restoration condition,
- structural stability,
- and apical findingstogether rather than relying on pain alone.
What This Means
The important question is not simply:
“Was the root canal done years ago?”
but:
“Has long-term biologic and structural stability been maintained?”
A root canal treated tooth continues functioning within:
- a bacterial environment,
- ongoing chewing and biting forces,
- restorative wear,
- and long-term structural loading.
Over time:
- bacterial leakage,
- unresolved anatomy,
- crack propagation,
- or restorative breakdownmay alter the long-term prognosis.
Modern evaluation increasingly focuses on:
- biologic stability,
- restoration integrity,
- and longitudinal monitoringrather than assuming prior treatment guarantees permanent stability.
When to See a Dentist
You should consider evaluation if:
- a previously treated tooth begins hurting again,
- swelling develops near the tooth,
- chewing or biting becomes uncomfortable,
- a crown or filling loosens,
- gum drainage appears,
- or pressure sensitivity returns unexpectedly.
Previously treated teeth may require reassessment even years later.
- apical healing,
- restoration integrity,
- crack risk,
- bacterial leakage,
- and structural prognosis—not just whether the tooth had prior treatment.
Early evaluation may improve the chances of preserving the tooth predictably long term.
Clinical Perspective
For dental professionalsThis section discusses clinical reasoning and is not intended for self-diagnosis.
Late Endodontic Failure – Reinfection, Structural Compromise, and Persistent Apical Disease
Clinical Takeaway
Late root canal failure commonly reflects:
- microbial persistence or reinfection,combined with:
- long-term structural and restorative compromiserather than a single isolated procedural event.
Interpretation Framework
Delayed endodontic failure should be interpreted as a dynamic interaction between:
- microbial control durability,
- coronal seal integrity,
- structural fatigue,
- missed anatomy,
- and host healing response.
Clinical assessment requires integration of:
- symptom recurrence,
- restoration integrity,
- apical radiographic findings,
- periodontal status,
- fracture-risk assessment,
- prior treatment complexity,
- and longitudinal healing behavior.
The key challenge is distinguishing:
stable post-treatment adaptation
from:
biologic reinfection or structural decompensation.
Current interpretation increasingly emphasizes:
- longitudinal prognosis behavior,
- structural-restorative durability,
- and biologic stability monitoring.
Current Understanding (Guidelines + Evidence)
Endodontic Perspective (AAE / ESE Aligned)
Late failure mechanisms commonly include:
- coronal leakage,
- missed canal anatomy,
- persistent intraradicular infection,
- vertical root fracture,
- recurrent decay,
- and unresolved apical inflammation.
Important interpretation principles include:
- successful healing may remain stable for years before reinfection occurs,
- restoration quality strongly influences long-term survival,
- structural integrity is often as important as canal disinfection,
- and asymptomatic apical recurrence remains possible.
Biologic Insight
Bacterial recolonization through coronal leakage may:
- reactivate apical inflammation,
- re-establish microbial biofilms,
- and destabilize previously healed lesions.
Persistent biofilm niches may survive:
- initial treatment,
- inaccessible anatomy,
- or long-term restoration breakdown.
Additionally:
- cyclic occlusal loading,
- structural fatigue,
and crack propagationcontribute to delayed biomechanical compromise.
Differential Diagnosis
1. Persistent Apical Periodontitis
Features:
- unresolved lesion,
- microbial persistence,
- incomplete healing.
2. Secondary Reinfection
Features:
- restoration breakdown,
- coronal leakage,
- recurrent bacterial ingress.
3. Vertical Root Fracture
Features:
- isolated probing defect,
- localized inflammation,
- poor long-term prognosis.
4. Occlusal / Structural Overload
Features:
- crack propagation,
- ligament inflammation,
- chewing or biting tenderness.
Key Diagnostic Distinctions
| Feature | Stable Treated Tooth | Delayed Failure Concern |
|---|---|---|
| Symptoms | Minimal/absent | Recurring/persistent |
| Apical findings | Stable/healed | Enlarging lesion possible |
| Restoration integrity | Intact | Breakdown/leakage |
| Structural stability | Preserved | Crack risk increased |
| Periodontal findings | Stable | Localized changes possible |
Common Pitfalls
Common diagnostic errors include:
- assuming prior RCT excludes future pathology,
- missing vertical root fractures,
- overlooking coronal leakage,
- interpreting asymptomatic lesions as stable without monitoring,
- and failure to reassess restorability during retreatment planning.
Long-term interpretation should always integrate:
- biologic stability,
- restoration durability,
- and structural prognosis.
Emerging Research Directions
Endodontic Retreatment Analytics
Research increasingly focuses on:
- persistent infection mapping,
- biofilm persistence characterization,
- structural fatigue prediction,
- and retreatment prognostic analytics.
AI-Assisted Interpretation
Emerging systems increasingly evaluate:
- reinfection-risk modeling,
- apical healing analytics,
- retreatment prognosis prediction,
- and longitudinal structural-risk assessment.
Advanced Imaging Integration
Current research increasingly explores:
- CBCT-based missed anatomy detection,
- fracture-risk analysis,
- longitudinal lesion progression tracking,
- and structural-restorative interaction modeling.
AI Potential
Delayed root canal failure represents a:
- longitudinal prognosis interpretation problemwhere:
- microbial control,
- structural integrity,
- and restorative durabilityinteract over years.
AI can assist across the clinical workflow:
Interpretation
- Integrating imaging, restoration condition, symptom recurrence, and apical findings
- Identifying clinically meaningful reinfection and structural-failure patterns
Decision Timing
- Supporting retreatment versus extraction planning
- Flagging high-risk leakage or fracture presentations
- Assisting long-term monitoring strategies
Patient Communication
- Explaining why previously treated teeth may develop problems years later
- Clarifying the importance of restoration integrity and long-term maintenance
- Improving understanding of retreatment rationale
Clinical Workflow Support
- Structuring long-term endodontic reassessment consistently
- Supporting longitudinal healing tracking
- Reducing variability in retreatment interpretation
Emerging Direction
- AI-assisted long-term endodontic prognosis modeling
- Predictive coronal-leakage analytics
- Integrated structural and biologic retreatment-risk systems
Clinical Relevance
The challenge is not simply identifying recurrent symptoms — it is determining whether long-term biologic stability has failed because of:
- reinfection,
- unresolved anatomy,
- or progressive structural compromise.
AI may eventually help:
- improve interpretation of delayed endodontic failure,
- support earlier recognition of reinfection risk,
- reduce variability in retreatment planning,
- and enhance patient communication regarding long-term tooth preservation.
References
- European Society of Endodontology (ESE). Quality guidelines for endodontic treatment. International Endodontic Journal.
- Ng YL, Mann V, Gulabivala K. Outcome of primary root canal treatment: systematic review of the literature. Part 2. Influence of clinical factors. International Endodontic Journal.
- Siqueira JF Jr, Rôças IN. Clinical implications and microbiology of bacterial persistence after treatment procedures. Journal of Endodontics.
- Ray HA, Trope M. Periapical status of endodontically treated teeth in relation to the technical quality of the root filling and the coronal restoration. International Endodontic Journal.
- Ricucci D, Siqueira JF Jr. Recurrent apical periodontitis and late endodontic treatment failure related to coronal leakage: a case report. Journal of Endodontics.
- Fuss Z, Lustig J, Tamse A. Prevalence of vertical root fractures in extracted endodontically treated teeth. International Endodontic Journal.
- Song M, Kim HC, Lee W, Kim E. Analysis of the cause of failure in nonsurgical endodontic treatment by microscopic inspection during endodontic microsurgery. Journal of Endodontics.
- Aminoshariae A, Kulild J, Nagendrababu V. Artificial Intelligence in Endodontics: Current Applications and Future Directions. J Endod.