How many sittings does root canal treatment need?
The number of root canal sittings depends less on a fixed rule and more on the condition of the tooth, infection status, and treatment complexity



Short Answer
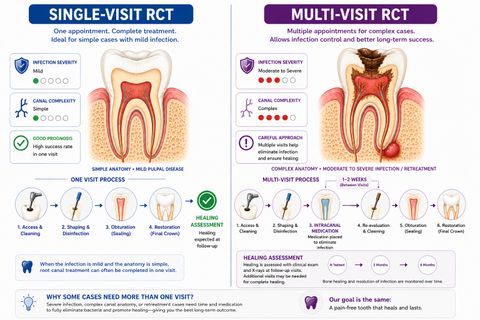
Root canal treatment may sometimes be completed in a single visit, while other cases require multiple sittings. The number of appointments depends on factors such as infection severity, pain, swelling, tooth anatomy, retreatment complexity, and how the tooth responds during treatment.
Can Root Canal Treatment Be Done in One Sitting?
Yes — some root canal treatments can be completed in:
- one sitting,especially when:
- infection is limited,
- symptoms are controlled,
- and the canal system can be disinfected effectively in a single appointment.
People are often surprised that:
- some teeth need one visit,while:
- others require two or more appointments.
This difference does not automatically mean:
- one tooth is “better” or “worse.”
Why Do Some Teeth Need Multiple Visits?
The number of sittings depends on factors such as:
- infection severity,
- swelling or drainage,
- tooth anatomy,
- number and shape of canals,
- retreatment complexity,
- and patient comfort during treatment.
Dentists sometimes prefer multiple visits when:
- infection is extensive,
- swelling or drainage persists,
- canals are difficult to disinfect fully,
- or medication placement between visits may improve microbial control.
In some cases:
- additional visits help improve:
- infection control,
- symptom stabilization,
- and long-term healing predictability.
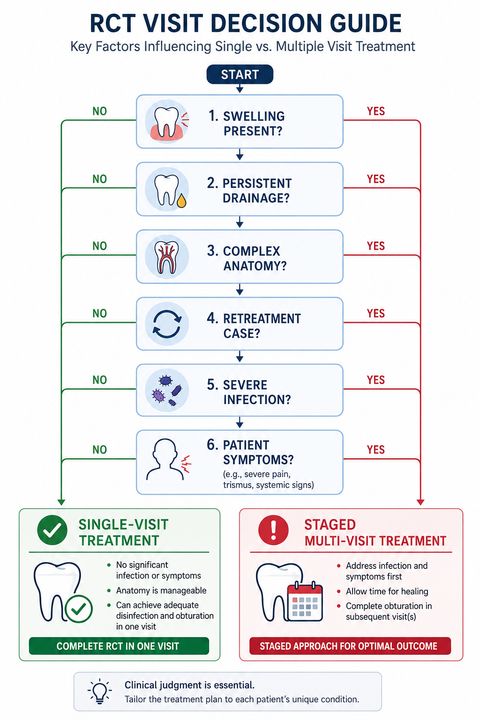
Single-Visit vs Multi-Visit Treatment
| Situation | More Likely Single Visit | More Likely Multiple Visits |
|---|---|---|
| Infection severity | Lower | Higher |
| Swelling or drainage | Minimal | Persistent |
| Canal anatomy | Simpler | More complex |
| Retreatment case | Less common | More common |
| Disinfection predictability | Higher | Reduced |
| Symptom severity | Mild/moderate | Severe or unstable |
Importantly:
- more sittings do not automatically mean the tooth is worse,and:
- fewer sittings do not necessarily mean the treatment is biologically simpler.
What This Means
The important question is not simply:
“How many appointments are needed?”
but:
“Can the infection and canal system be managed predictably and safely?”
- infection status,
- structural complexity,
- symptom behavior,
- healing response,
- and disinfection predictabilitytogether rather than following a fixed number-of-visits rule.
Some teeth respond quickly and predictably.
Others require:
- staged treatment,
- intracanal medication,
- or reassessment between visitsto improve long-term treatment success.
When to See a Dentist
You should consider evaluation if:
- tooth pain or swelling develops,
- chewing or biting becomes uncomfortable,
- symptoms return between visits,
- temporary fillings break,
- or swelling or drainage persists.
The number of appointments may change depending on:
- how the tooth responds during treatment,
- symptom progression,
- and infection control.
- infection control,
- canal anatomy,
- healing response,
- structural condition,
- and treatment complexity—not just whether treatment was completed in one visit.
Proper follow-up helps improve long-term treatment success.
Related Questions
Clinical Perspective
For dental professionalsThis section discusses clinical reasoning and is not intended for self-diagnosis.
Single-Visit vs Multi-Visit Endodontic Treatment
Clinical Takeaway
The decision between single-visit and multi-visit root canal treatment depends on:
- infection status,
- canal disinfection predictability,
- structural complexity,
- and biologic controlrather than procedural preference alone.
Interpretation Framework
Visit number should be interpreted as a:
- biologic,
- microbiologic,
- and procedural management decisionrather than a fixed protocol variable.
Clinical assessment requires integration of:
- pulpal/apical diagnosis,
- microbial burden,
- drainage status,
- canal anatomy complexity,
- retreatment considerations,
- patient tolerance,
- restorability,
- and long-term prognosis.
The key question is whether:
- predictable disinfection and biologic controlcan be achieved safely within a single appointment.
Current interpretation increasingly emphasizes:
- complexity-based planning,
- infection-control predictability,
- and prognosis-oriented treatment sequencing.
Current Understanding (Guidelines + Evidence)
Endodontic Perspective (AAE / ESE Aligned)
Single-visit treatment may be appropriate in:
- vital pulp cases,
- controlled infection states,
- straightforward anatomy,
- and asymptomatic or minimally symptomatic presentations.
Multi-visit treatment may be preferred in:
- persistent exudation or drainage,
- extensive apical pathology,
- retreatment cases,
- difficult canal disinfection scenarios,
- and severe symptomatic infection.
Important interpretation principles include:
- both approaches demonstrate high success when appropriately selected,
- case selection is more important than rigid protocol preference,
- intracanal medication may improve microbial control in selected cases,
- and procedural quality remains more significant than visit count alone.
Biologic Insight
Persistent microbial load and inflammatory activity influence:
- healing predictability,
- disinfection complexity,
- and symptom stabilization.
- improved microbial control,
- reduction of inflammatory burden,
- and better management of persistent drainage or exudation.
Differential Diagnosis
1. Vital Pulp Therapy / Straightforward Primary RCT
Features:
- often suitable for single visit,
- limited microbial burden,
- predictable canal management.
2. Necrotic Tooth with Apical Periodontitis
Features:
- may require staged disinfection,
- variable symptom behavior,
- healing-risk considerations.
3. Acute Apical Abscess
Features:
- drainage management important,
- symptom stabilization may require multiple visits,
- inflammatory burden elevated.
4. Retreatment Case
Features:
- complex anatomy,
- persistent infection risk,
- increased procedural uncertainty,
- staged management commonly considered.
Key Diagnostic Distinctions
| Factor | Single-visit tendency | Multi-visit tendency |
|---|---|---|
| Infection severity | Lower | Higher |
| Drainage/exudate | Minimal | Persistent |
| Anatomy complexity | Simpler | More complex |
| Retreatment status | Less common | More common |
| Disinfection predictability | Higher | Reduced |
| Procedural uncertainty | Lower | Higher |
Common Pitfalls
Common diagnostic errors include:
- assuming single-visit treatment is universally superior,
- overextending treatment despite uncontrolled infection,
- underestimating retreatment complexity,
- inadequate temporization between visits,
- and confusing procedural convenience with biologic suitability.
Visit planning should always integrate:
- microbiologic control,
- structural prognosis,
- and procedural predictability.
Emerging Research Directions
Disinfection Optimization
Research increasingly focuses on:
- irrigant activation systems,
- biofilm disruption technologies,
- intracanal antimicrobial strategies,
- and advanced canal-cleaning protocols.
AI-Assisted Treatment Planning
Emerging systems increasingly evaluate:
- anatomy complexity prediction,
- procedural difficulty modeling,
- prognosis-oriented visit planning,
- and retreatment-risk analytics.
Outcome Analytics
Current research increasingly explores:
- biologic healing prediction,
- symptom-resolution modeling,
- and retreatment-risk stratification.
AI Potential
The decision between single-visit and multi-visit root canal treatment represents a procedural-biologic interpretation problem where clinical meaning depends on:
- infection control,
- anatomy complexity,
- and healing predictability.
AI can assist across the clinical workflow:
Interpretation
- Integrating imaging, anatomy complexity, symptom behavior, and infection status
- Identifying clinically meaningful disinfection-risk patterns
Decision Timing
- Supporting single-visit versus staged-treatment decisions
- Flagging retreatment or persistent-infection complexity
- Assisting prognosis-oriented procedural planning
Patient Communication
- Explaining why some teeth require multiple visits
- Clarifying infection-control and healing considerations
- Improving understanding of staged-treatment rationale
Clinical Workflow Support
- Structuring treatment-complexity assessment
- Supporting longitudinal infection management
- Reducing variability in procedural decision-making
Emerging Direction
- AI-assisted anatomy-complexity prediction
- Predictive disinfection modeling
- Multimodal treatment-planning analytics integrating imaging and clinical findings
Clinical Relevance
The challenge is not simply deciding the number of visits — it is determining how to achieve:
- predictable biologic control,
- effective canal disinfection,
- and long-term healingbased on the specific disease state and structural complexity of the tooth.
AI may eventually help:
- improve procedural planning,
- support complexity-based visit selection,
- reduce variability in endodontic management,
- and enhance patient communication regarding treatment sequencing.
References
- European Society of Endodontology (ESE). Quality guidelines for endodontic treatment. International Endodontic Journal.
- Sathorn C, Parashos P, Messer H. Effectiveness of single- versus multiple-visit endodontic treatment of teeth with apical periodontitis: a systematic review and meta-analysis. International Endodontic Journal.
- Figini L, Lodi G, Gorni F, Gagliani M. Single versus multiple visits for endodontic treatment of permanent teeth. Cochrane Database of Systematic Reviews.
- Sjögren U, Figdor D, Persson S, Sundqvist G. Influence of infection at the time of root filling on the outcome of endodontic treatment of teeth with apical periodontitis. International Endodontic Journal.
- Peters OA. Current challenges and concepts in the preparation of root canal systems: a review. Journal of Endodontics.
- Siqueira JF Jr, Rôças IN. Clinical implications and microbiology of bacterial persistence after treatment procedures. Journal of Endodontics.
- Ng YL, Mann V, Gulabivala K. Outcome of primary root canal treatment: systematic review of the literature. Part 2. Influence of clinical factors. International Endodontic Journal.
- Schwendicke F, Samek W, Krois J. Artificial intelligence in dentistry: chances and challenges. Journal of Dental Research.