Can Stress Cause Tooth Pain?
Stress may not directly create cavities or infection, but it can increase muscle tension, clenching, grinding, and pain sensitivity around the teeth and jaw.



Short Answer
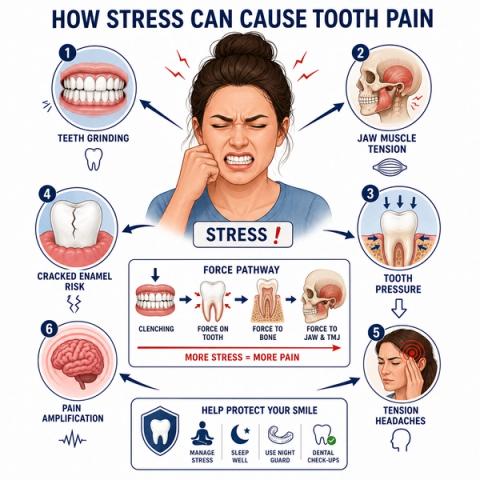
Yes, stress can sometimes contribute to tooth pain indirectly. Stress-related clenching, grinding, muscle tension, and heightened pain sensitivity may create pressure on teeth, supporting tissues, and jaw muscles, leading to discomfort that can feel similar to dental pain. Stress can also worsen symptoms from already irritated or structurally vulnerable teeth.
How Can Stress Affect Teeth and Jaw Pain?
Stress can affect the mouth and jaw in several ways.
Some people unconsciously:
- clench their teeth,
- grind during sleep,
- tighten jaw muscles,
- or overload certain teeth during stressful periods or poor sleep.
Over time, this may create:
- tooth soreness,
- pressure sensitivity,
- jaw discomfort,
- headaches,
- chewing or biting fatigue,
- or crack-related irritation.
People commonly describe it as:
- “My teeth feel sore in the morning.”
- “My jaw feels tight.”
- “Pain shifts between different teeth.”
- “Chewing feels tiring.”
- “My teeth feel sensitive but nothing looks wrong.”
- “Stress seems to make the pain worse.”
Stress may also:
- increase awareness of pain,
- amplify existing sensitivity,
- or worsen symptoms from already inflamed teeth.
What Happens During Stress-Related Tooth Pain?
Stress itself does not directly cause:
- cavities,
- pulpal infection,
- or bacterial tooth decay.
However:stress-related muscle tension and grinding can place excessive force on:
- teeth,
- periodontal ligaments,
- jaw muscles,
- and existing cracks or restorations.
Repeated clenching or grinding may contribute to:
- pressure sensitivity,
- structural fatigue,
- crack progression,
- jaw soreness,
- and tooth discomfort during chewing or biting.
Some people may also develop:
- facial muscle fatigue,
- headaches,
- or pain that shifts location rather than remaining localized to one tooth.
Why the Pattern of Pain Matters
| Pain Pattern | What It May Suggest |
|---|---|
| Morning tooth soreness | Night grinding or clenching |
| Jaw tightness or fatigue | Muscle overactivity |
| Pain shifting between teeth | Muscular or parafunctional pattern |
| Pain during chewing or biting | Pressure-related overload |
| Worn teeth or flattening | Bruxism-related stress |
| Sharp pain in one tooth | Possible crack or true dental disease |
| Lingering heat or cold pain | Possible pulpal involvement |
Dentists evaluate:
- bite patterns,
- muscle tenderness,
- tooth wear,
- crack risk,
- pulpal findings,
and symptom distributionrather than attributing symptoms to stress alone.

What This Means
Stress-related tooth pain is often:
- mechanical,
- muscular,
- pressure-related,
- or pain-amplification relatedrather than directly infectious.
However:persistent tooth pain should not automatically be assumed to be “just stress.”
Stress may:
- worsen symptoms from already inflamed teeth,
- amplify crack-related discomfort,
- or increase awareness of underlying dental problems.
The important question is not simply:
“Am I stressed?”
but:
“What tissues are actually producing the pain?”
A proper evaluation helps determine whether symptoms are:
- muscular,
- structural,
- inflammatory,
- or a combination of these factors.
When to See a Dentist
You should consider evaluation if:
- teeth feel sore or sensitive repeatedly,
- jaw tightness develops,
- headaches occur with tooth discomfort,
- chewing or biting becomes uncomfortable,
- teeth appear worn or cracked,
- or pain persists or worsens over time.
Stress-related clenching may coexist with:
- cracked teeth,
- pulpal inflammation,
- or actual dental disease.
A dentist evaluates:
- tooth wear,
- bite stress,
- crack patterns,
- muscle tenderness,
- pulpal status,
- and symptom progression—not just emotional stress levels.
Early evaluation may help prevent structural damage from chronic grinding or clenching.
Clinical Perspective
For dental professionalsThis section discusses clinical reasoning and is not intended for self-diagnosis.
Stress-Related Dental Pain – Bruxism, Muscle Tension, and Pain Amplification
Clinical Takeaway
Stress-related dental pain commonly emerges through parafunctional loading, masticatory muscle hyperactivity, central pain modulation changes, and secondary structural consequences rather than direct odontogenic disease alone.
Interpretation Framework
Stress-associated tooth pain should be interpreted as a multifactorial interaction involving:
- biomechanical overload,
- muscular tension,
- nociceptive amplification,
- structural fatigue,
- and existing dental vulnerability.
Clinical assessment requires integration of:
- parafunctional behavior,
- occlusal wear patterns,
- muscle tenderness,
- crack-risk findings,
- pulpal testing,
- symptom distribution,
- and psychosocial context.
The key challenge is distinguishing:
- non-odontogenic stress-amplified pain,from:
- true pulpal or structural pathology exacerbated by parafunction.
Current interpretation increasingly emphasizes:
- biomechanical-functional overlap,
- central sensitization contribution,
- and multimodal pain behaviorrather than isolated symptom localization.
Current Understanding (Guidelines + Evidence)
Orofacial Pain / Restorative Perspective
Stress-related dental symptoms commonly involve:
- bruxism-related loading,
- masticatory muscle tension,
- occlusal overload,
- crack propagation risk,
- and heightened pain sensitivity.
Important interpretation principles include:
- stress may amplify existing nociceptive input,
- parafunction can produce periodontal ligament soreness and structural fatigue,
- generalized shifting discomfort patterns are less typical of localized pulpal disease,
- and true odontogenic pathology may coexist simultaneously.
Biomechanical Insight
Repetitive occlusal loading increases:
- microstrain within enamel and dentin,
- periodontal ligament compression,
- and structural fatigue accumulation.
Chronic muscular hyperactivity may also alter:
- craniofacial pain distribution,
- referred pain patterns,
- and pain amplification behavior.
Differential Diagnosis
1. Bruxism-Associated Pain
Features:
- morning soreness,
- generalized pressure sensitivity,
- tooth wear patterns,
- muscular fatigue.
2. Cracked Tooth Syndrome
Features:
- stress-amplified structural symptoms,
- intermittent biting pain,
- localized sensitivity,
- load-dependent discomfort.
3. Myofascial Referred Pain
Features:
- diffuse aching,
- muscle trigger-point referral,
- non-localized dental discomfort,
- variable pain distribution.
4. True Pulpal Disease with Stress Amplification
Features:
- localized thermal findings,
- inflammatory pain,
- symptom intensification during stress periods,
- mixed mechanical and inflammatory behavior.
Key Diagnostic Distinctions
| Feature | Stress-Related Pain | Odontogenic Inflammatory Pain |
|---|---|---|
| Localization | More diffuse/variable | More localized |
| Thermal sensitivity | Less characteristic | More characteristic |
| Muscle tenderness | More common | Less central |
| Tooth wear/clenching signs | Frequent | Variable |
| Spontaneous throbbing | Less typical | More concerning |
| Pain shifting between teeth | More common | Less typical |
Common Pitfalls
Common diagnostic errors include:
- dismissing true dental disease as stress alone,
- missing crack-related structural overload,
- overlooking muscular referral patterns,
- over-reliance on radiographs in parafunctional pain,
- and failure to assess psychosocial amplification factors.
Stress-related symptoms should always be correlated with:
- vitality testing,
- structural findings,
- and functional loading behavior.
Emerging Research Directions
Bruxism Analytics
Research increasingly focuses on:
- sleep-related parafunctional monitoring,
- occlusal force-pattern analysis,
- structural fatigue prediction,
- and wearable bruxism assessment systems.
AI-Assisted Interpretation
Emerging systems increasingly evaluate:
- multimodal orofacial pain classification,
- stress-amplification modeling,
- and parafunctional risk prediction.
Pain Neuroscience
Current research increasingly explores:
- central sensitization mapping,
- neuroinflammatory modulation,
- biopsychosocial dental pain integration,
- and muscular-pain amplification dynamics.
AI Potential
Stress-associated tooth pain represents a multimodal interpretation problem where biomechanical loading, muscular activity, and nociceptive amplification overlap with potential odontogenic disease.
AI can assist across the clinical workflow:
Interpretation
- Integrating wear patterns, muscle findings, symptom distribution, and pulpal testing
- Identifying clinically meaningful parafunctional versus inflammatory patterns
Decision Timing
- Supporting preventive intervention before structural fatigue progresses
- Flagging crack-risk and overload-risk presentations
- Assisting referral and monitoring decisions
Patient Communication
- Explaining how stress may affect teeth and jaw structures
- Clarifying differences between muscle-related pain and infection-related pain
- Improving understanding of parafunctional loading effects
Clinical Workflow Support
- Structuring parafunctional-risk assessment
- Supporting longitudinal symptom tracking
- Reducing variability in overlapping pain interpretation
Emerging Direction
- AI-assisted bruxism-risk prediction
- Integrated occlusal-load and pain-pattern analytics
- Predictive structural-fatigue modeling
Clinical Relevance
The challenge is not simply identifying stress exposure — it is determining whether parafunctional loading and pain amplification are producing symptoms independently or interacting with underlying dental pathology.
AI may eventually help:
- improve differentiation between stress-related and odontogenic pain,
- support earlier recognition of overload-related structural damage,
- reduce variability in parafunctional interpretation,
- and enhance patient communication regarding stress-related dental effects.
References
- Lobbezoo F, Ahlberg J, Glaros AG, et al. Bruxism defined and graded: an international consensus. Journal of Oral Rehabilitation.
- Manfredini D, Winocur E, Guarda-Nardini L, Paesani D, Lobbezoo F. Epidemiology of bruxism in adults: a systematic review of the literature. Journal of Orofacial Pain.
- Okeson JP. Management of Temporomandibular Disorders and Occlusion. Elsevier.
- American Academy of Orofacial Pain (AAOP). Orofacial Pain: Guidelines for Assessment, Diagnosis, and Management. Quintessence Publishing.
- Banerji S, Mehta SB, Millar BJ. Cracked tooth syndrome. Part 1: aetiology and diagnosis. British Dental Journal.
- Greene CS, Klasser GD, Epstein JB. Revision of the American Academy of Orofacial Pain taxonomy for temporomandibular disorders and orofacial pain. Journal of Oral & Facial Pain and Headache.
- Wieckiewicz M, Paradowska-Stolarz A, Wieckiewicz W. Psychosocial aspects of bruxism: the most paramount factor influencing teeth grinding. BioMed Research International.
- Schwendicke F, Samek W, Krois J. Artificial intelligence in dentistry: chances and challenges. Journal of Dental Research.