How to differentiate nerve pain vs gum pain?
Not all tooth pain comes from the tooth nerve itself — the pattern, trigger, and location of pain often reveal whether the source is pulpal or gum-related



Short Answer
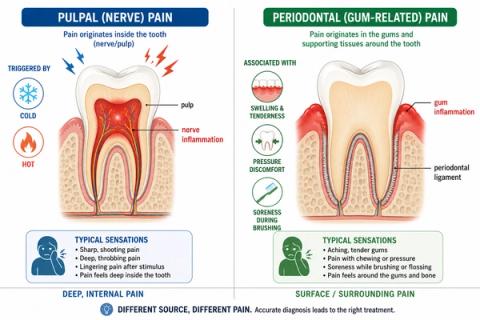
Tooth nerve pain usually feels deeper, sharper, temperature-sensitive, throbbing, or spontaneous, while gum-related pain is more commonly associated with soreness, swelling, pressure, or tenderness around the gums and supporting tissues. The difference depends more on how the pain behaves than where it is felt. Some conditions can also involve both the tooth nerve and surrounding gums at the same time.
What Is Tooth Nerve Pain?
Tooth nerve pain usually comes from inflammation or irritation inside the tooth.
People commonly describe it as:
- “A deep throbbing toothache.”
- “Sharp pain with cold drinks.”
- “Pain that lingers after eating or drinking.”
- “A toothache that wakes me at night.”
- “Pain that is hard to pinpoint exactly.”
- “Sudden spontaneous tooth pain.”
Nerve-related pain often becomes worse with:
What Is Gum-Related Tooth Pain?
Gum-related pain usually comes from the tissues surrounding and supporting the tooth.
People commonly describe it as:
- “My gums feel sore around the tooth.”
- “Pain while chewing or biting.”
- “Tenderness near the gumline.”
- “Swollen or bleeding gums.”
- “Pressure around the tooth.”
- “The tooth feels bruised when biting.”
Gum-related pain is more commonly associated with:
- swelling,
- tenderness,
- pressure,
- biting discomfort,
- and irritation around the gums or supporting bone.
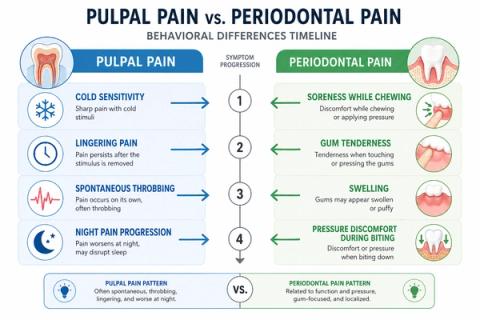
Why the Pattern of Pain Matters
| Pain Pattern | What It May Suggest |
|---|---|
| Sharp pain to cold or heat | Nerve-related pain |
| Lingering sensitivity | Pulp inflammation |
| Spontaneous throbbing pain | Deeper nerve irritation |
| Swelling near the gums | Gum-related inflammation |
| Pain during chewing or biting | Gum or root-area irritation |
| Localized soreness near gumline | Periodontal involvement |
| Difficulty identifying exact tooth | Pulpal pain referral |
| Bleeding gums with tenderness | Gum-related disease |
Symptoms can overlap, especially when both the tooth nerve and surrounding tissues are involved together.
What This Means
Pain location alone does not always identify the source of the problem.
For example:
- nerve pain can sometimes feel diffuse or spread across multiple teeth,
- while gum-related pain is often easier to localize near the gums or biting area.
In some cases:
- both the pulp and periodontal tissues become inflamed together,creating mixed symptoms that are difficult to interpret without testing.
Dentists therefore evaluate:
- triggers,
- sensitivity patterns,
- swelling,
- chewing or biting response,
- and tissue behavior togetherrather than relying on one symptom alone.
When to See a Dentist
You should consider evaluation if:
- pain becomes persistent,
- swelling or bleeding develops,
- temperature sensitivity lingers,
- chewing or biting becomes uncomfortable,
- pain wakes you from sleep,
- or the source of pain is difficult to identify.
Different causes of pain often require very different treatments.
A dentist may evaluate:
- vitality response,
- gum condition,
- probing findings,
- percussion response,
- and radiographic patternsto determine whether the source is pulpal, periodontal, or combined.
Related Questions
Clinical Perspective
For dental professionalsThis section discusses clinical reasoning and is not intended for self-diagnosis.
Pulpal Pain vs Periodontal Pain – Diagnostic Differentiation
Clinical Takeaway
Differentiating pulpal from periodontal pain requires interpretation of:
- symptom behavior,
- tissue response,
- localization quality,
- and stimulus characteristicsrather than relying on pain location alone.
Interpretation Framework
Pulpal and periodontal pain originate from distinct biologic mechanisms but frequently overlap clinically.
Interpretation requires integration of:
- thermal response,
- spontaneous pain behavior,
- localization characteristics,
- periodontal findings,
- percussion response,
- and progression pattern.
Pain origin may become difficult to distinguish in:
- combined endodontic-periodontal lesions,
- referred pulpal pain,
- or advanced inflammatory involvement.
Current interpretation increasingly emphasizes:symptom behavior and tissue response patterns over isolated descriptors.
Current Understanding (Guidelines + Evidence)
Endodontic Perspective (AAE / ESE Aligned)
Pulpal pain commonly demonstrates:
- thermal sensitivity,
- spontaneous episodes,
- lingering response,
- diffuse localization,
- and nocturnal exacerbation.
Periodontal pain more commonly demonstrates:
- localized tenderness,
- biting discomfort,
- swelling,
- probing-related findings,
- and palpation sensitivity.
Important interpretation principles:
- pulpal pain may refer across regions,
- periodontal pain is often more localized,
- and combined lesions may blur classic distinctions.
Neurophysiologic Insight
Pulpal nociception is heavily influenced by:
- confined inflammatory pressure,
- intrapulpal vascular changes,
- and neural sensitization.
Periodontal pain more commonly involves:
- mechanoreceptive loading,
- inflammatory response within supporting tissues,
- and periodontal ligament activation.
Differential Diagnosis
1. Symptomatic Irreversible Pulpitis
Features:
- lingering thermal pain,
- spontaneous throbbing,
- diffuse localization,
- possible nocturnal pain.
2. Symptomatic Apical Periodontitis
Features:
3. Periodontal Abscess
Features:
4. Combined Endodontic-Periodontal Lesion
Features:
Key Diagnostic Distinctions
| Feature | Pulpal pain | Periodontal pain |
|---|---|---|
| Thermal sensitivity | Common | Less characteristic |
| Localization | Diffuse | More localized |
| Swelling location | Usually late | More common earlier |
| Pain on probing | Variable | More characteristic |
| Spontaneous pain | Common | Less common |
| Biting discomfort | Variable | More common |
Common Pitfalls
Common diagnostic errors include:
- assuming localized pain excludes pulpal disease,
- missing combined endo-perio lesions,
- over-reliance on radiographs alone,
- failure to correlate probing with vitality findings,
- and misdiagnosing referred pulpal pain as periodontal disease.
Combined lesions frequently challenge classic symptom-pattern assumptions.
Emerging Research Directions
Pain-Pattern Analysis
Current research increasingly focuses on:
- symptom-behavior modeling,
- integration of thermal and periodontal findings,
- and probabilistic diagnostic interpretation.
Imaging Advancements
Emerging work includes:
- AI-assisted radiographic interpretation,
- periodontal defect pattern recognition,
- and pulpal-periapical correlation analysis.
Biologic Profiling
Research directions increasingly explore:
- inflammatory biomarker differentiation,
- host-response characterization,
- and tissue-specific inflammatory signatures.
AI Potential
Differentiating nerve pain from gum-related pain represents a multi-factor interpretation problem where clinical meaning emerges from combining symptom behavior, tissue response, and structural findings.
AI can assist across the clinical workflow:
Interpretation
- Integrating thermal response, probing findings, percussion response, and symptom history
- Identifying clinically meaningful pulpal vs periodontal patterns
Decision Timing
- Supporting referral and treatment-sequencing decisions
- Flagging combined lesion risk patterns
- Assisting in ambiguous presentations
Patient Communication
- Explaining why different tissues produce different pain behaviors
- Clarifying why additional testing is needed
- Improving understanding of treatment rationale
Clinical Workflow Support
- Structuring endodontic-periodontal findings systematically
- Supporting consistent diagnostic interpretation
- Reducing variability in symptom assessment
Emerging Direction
- AI-assisted endo-perio differentiation
- Multimodal symptom-imaging integration
- Predictive modeling of combined lesion progression
Clinical Relevance
The challenge is not simply identifying dental pain — it is determining whether the origin is pulpal, periodontal, or combined, and selecting the correct intervention pathway.
AI may eventually help:
- improve interpretation of overlapping pain patterns,
- support earlier differentiation of tissue origin,
- reduce diagnostic variability,
- and enhance patient communication clarity.
References
- European Society of Endodontology (ESE). Quality Guidelines for Endodontic Treatment. International Endodontic Journal. 2023.
- American Association of Endodontists (AAE). Endodontic Diagnosis. AAE Clinical Resources.
- Simon JHS, Glick DH, Frank AL. The relationship of endodontic-periodontic lesions. Journal of Periodontology.
- Rotstein I, Simon JHS. Diagnosis, prognosis and decision-making in the treatment of combined periodontal-endodontic lesions. Periodontology 2000.
- Ricucci D, Siqueira JF Jr, Rôças IN. Pulp Response to Periodontal Disease: Novel Observations Help Clarify the Processes of Tissue Breakdown and Infection. J Endod.
- Hargreaves KM, Berman LH. Cohen’s Pathways of the Pulp. Elsevier.
- Herrera D, Retamal-Valdes B, Alonso B, Feres M. Acute periodontal lesions (periodontal abscesses and necrotizing periodontal diseases) and endodontic-periodontal lesions. Journal of Clinical Periodontology.
- Chen Z, Huang H, Pan X, et al. Artificial intelligence in pulpal and periapical diagnosis: current status and future directions. International Endodontic Journal.