Why Does My Tooth Hurt After a Filling?
Some sensitivity after a filling can be temporary, but persistent or worsening pain may indicate deeper pulpal or bite-related irritation.



Short Answer
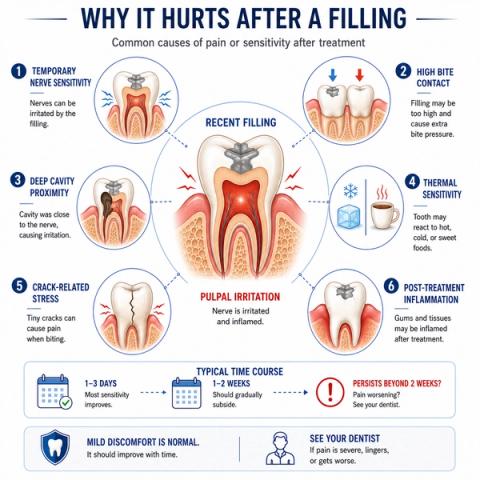
A tooth may hurt after a filling because the nerve inside the tooth becomes temporarily irritated during treatment or because bite pressure changes slightly after the restoration. In some cases, deeper pulpal inflammation, cracks, or high bite contact may contribute to persistent discomfort. Mild sensitivity after a filling can be normal initially, but worsening or lingering pain deserves reassessment.
Is Tooth Sensitivity After a Filling Normal?
Yes — it is not uncommon for a tooth to feel different for a short period after a filling.
People commonly notice:
- cold sensitivity,
- mild chewing or biting discomfort,
- pressure sensitivity,
- brief sharp sensations,
- or awareness of the tooth while chewing.
This may happen because:
- the tooth nerve was already irritated before treatment,
- drilling and restoration temporarily stimulate the pulp,
- bite pressure changes slightly after the filling,
- or deep decay existed close to the nerve.
In many cases:
- mild sensitivity gradually improves over days or weeks.
Why Does a Tooth Hurt After a Filling?
A filling changes both:
- the structure of the tooth,and:
- how force travels through it during chewing or biting.
Post-restorative discomfort may occur because:
- the pulp temporarily reacts to treatment,
- dentin becomes more sensitive,
- the bite sits slightly high,
- or the tooth was already close to irreversible inflammation before treatment.
People may notice:
- cold sensitivity,
- pain while chewing or biting,
- pressure-related soreness,
- or occasional throbbing discomfort.
In some cases:
- cracks or structural weakness become more noticeable after restoration-related stress changes.
Why the Pattern of Pain Matters
| Pain Pattern | What It May Suggest |
|---|---|
| Mild cold sensitivity improving gradually | Normal postoperative adaptation |
| Pain while chewing or biting | High bite or structural stress |
| Lingering cold or heat pain | Deeper pulpal inflammation |
| Spontaneous throbbing pain | Advanced pulpal irritation |
| Bite feels uneven | Occlusal discrepancy |
| Symptoms worsening over time | Progressive pulpal compromise |
- symptom duration,
- bite response,
- thermal behavior,
- restoration depth,
- vitality findings,
- and crack riskrather than assuming all post-filling pain is normal.
What This Means
Some post-filling sensitivity represents:
- temporary biologic adaptation,while:persistent or worsening symptoms may indicate:
- deeper pulpal inflammation,
- high bite pressure,
- crack-related stress,
- or incomplete recovery of the tooth nerve.
The important question is not simply:
“Does the tooth hurt after the filling?”
but:
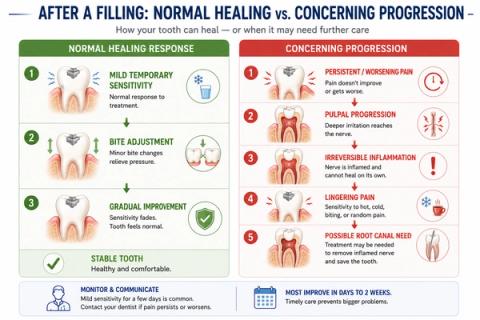
“Is the tooth improving or progressively worsening over time?”
Symptoms that gradually improve are usually less concerning than symptoms that:
- intensify,
- linger longer,
- become spontaneous,
- or spread into chewing and biting discomfort.
When to See a Dentist
You should consider evaluation if:
- sensitivity persists beyond a few weeks,
- pain worsens instead of improving,
- chewing or biting becomes painful,
- heat sensitivity develops,
- spontaneous throbbing pain appears,
- or the bite feels uneven.
A dentist evaluates:
- bite alignment,
- restoration fit,
- pulpal vitality,
- crack risk,
- and symptom progression—not just whether a filling was recently placed.
Early reassessment may help prevent progression toward more advanced pulpal disease.
Clinical Perspective
For dental professionalsThis section discusses clinical reasoning and is not intended for self-diagnosis.
Post-Restorative Tooth Pain – Pulpal Irritation and Occlusal Adaptation
Clinical Takeaway
Post-filling pain commonly reflects transient pulpal inflammatory response, occlusal overload, dentin permeability changes, or pre-existing pulpal compromise, but persistent symptoms require reassessment for irreversible progression or structural instability.
Interpretation Framework
Post-restorative sensitivity should be interpreted as a biologic and biomechanical response problem rather than a single-cause complication.
Clinical assessment requires integration of:
- restoration depth,
- preoperative pulpal status,
- occlusal contacts,
- thermal response,
- symptom trajectory,
- crack-risk findings,
- and restorative material behavior.
The key challenge is distinguishing:
- expected transient postoperative sensitivity,from:
- progressive pulpal decompensation or structural pathology.
Current interpretation increasingly emphasizes:
- temporal symptom progression,
- occlusal loading behavior,
- and pulpal recovery dynamicsrather than isolated postoperative discomfort.
Current Understanding (Guidelines + Evidence)
Restorative / Endodontic Perspective
Transient postoperative sensitivity may occur due to:
- dentin exposure,
- pulpal inflammatory activation,
- bonding-related permeability changes,
- and occlusal adaptation.
Persistent or worsening pain raises concern for:
- symptomatic irreversible pulpitis,
- occlusal trauma,
- crack propagation,
- or incomplete caries-related pulpal recovery.
Important interpretation principles include:
- preoperative pulpal condition strongly influences postoperative behavior,
- deep restorations increase inflammatory risk,
- symptom trajectory is more informative than isolated early sensitivity,
- and bite discrepancies commonly contribute to chewing discomfort.
Biologic Insight
Operative procedures alter:
- dentin-pulp fluid dynamics,
- dentinal permeability,
- and inflammatory mediator behavior.
Occlusal overload may additionally increase:
- periodontal ligament compression,
- mechanosensory activation,
- and structural stress around restored cusps.
Differential Diagnosis
1. Transient Postoperative Sensitivity
Features:
- mild thermal response,
- improving trajectory,
- limited spontaneous pain.
2. High Occlusion
Features:
- chewing or biting discomfort,
- pressure sensitivity,
- localized ligament inflammation,
- uneven bite perception.
3. Symptomatic Irreversible Pulpitis
Features:
- lingering thermal pain,
- spontaneous symptoms,
- worsening inflammatory progression,
- nocturnal discomfort possible.
4. Cracked Tooth with Restoration-Related Stress
Features:
- inconsistent bite pain,
- structural instability,
- variable thermal findings,
- stress-concentration behavior.
Key Diagnostic Distinctions
| Feature | Expected Postoperative Response | Concerning Pulpal Progression |
|---|---|---|
| Symptom trend | Improving | Worsening/persistent |
| Thermal response | Brief | Lingering |
| Spontaneous pain | Minimal | More concerning |
| Bite discomfort | Mild/transient | Increasing/persistent |
| Night pain | Uncommon | More concerning |
| Occlusal awareness | Temporary | Persistent/increasing |
Common Pitfalls
Common diagnostic errors include:
- reassuring persistent worsening symptoms prematurely,
- missing high occlusal contacts,
- overlooking pre-existing pulpal compromise,
- failure to reassess deep restorations,
- and misattributing crack-related pain to routine sensitivity.
Post-restorative pain should always be interpreted within:
- preoperative pulpal context,
- structural condition,
- and symptom trajectory.
Emerging Research Directions
Restorative Biomaterials
Research increasingly focuses on:
- pulpal-protective adhesives,
- bioactive restorative systems,
- dentin-sealing technologies,
- and stress-distribution optimization.
AI-Assisted Interpretation
Emerging systems increasingly evaluate:
- postoperative symptom-risk prediction,
- pulpal decompensation forecasting,
- and occlusal overload analytics.
Advanced Vitality Diagnostics
Current research increasingly explores:
- physiologic pulpal perfusion assessment,
- inflammatory-state monitoring,
- and postoperative healing analytics.
AI Potential
Pain after a filling represents a progression-interpretation problem where postoperative biologic adaptation, structural loading, and pre-existing pulpal status interact dynamically.
AI can assist across the clinical workflow:
Interpretation
- Integrating symptom trajectory, restoration depth, thermal behavior, and bite findings
- Identifying clinically meaningful postoperative versus progressive inflammatory patterns
Decision Timing
- Supporting monitor versus intervene decisions
- Flagging risk of irreversible pulpal progression
- Assisting occlusal reassessment planning
Patient Communication
- Explaining why some sensitivity after fillings can be temporary
- Clarifying warning signs of deeper pulpal involvement
- Improving understanding of healing versus progression patterns
Clinical Workflow Support
- Structuring postoperative reassessment consistently
- Supporting longitudinal symptom tracking
- Reducing variability in postoperative pain interpretation
Emerging Direction
- AI-assisted postoperative pulpal-risk prediction
- Integrated occlusal-load and symptom analytics
- Predictive restorative-outcome modeling
Clinical Relevance
The challenge is not simply identifying pain after a filling — it is determining whether the tooth is undergoing normal biologic adaptation or progressing toward irreversible inflammatory compromise.
AI may eventually help:
- improve interpretation of postoperative symptoms,
- support earlier recognition of pulpal decompensation,
- reduce variability in restorative follow-up assessment,
- and enhance patient communication regarding expected recovery patterns.
References
- Brännström M. Dentin and pulp in restorative dentistry. Dental Therapeutics AB.
- Ritter AV, Boushell LW, Walter R. Sturdevant’s Art and Science of Operative Dentistry. Elsevier.
- American Association of Endodontists (AAE). Endodontic Diagnosis. AAE Clinical Resources.
- Bergenholtz G, Axelsson S, Davidson T, et al. Treatment of pulps in teeth affected by deep caries — a systematic review of the literature. International Endodontic Journal.
- Hilton TJ. Keys to clinical success with pulp capping: a review of the literature. Operative Dentistry.
- Krämer N, Frankenberger R. Clinical performance of bonded posterior composite restorations. Quintessence International.
- Opdam NJM, Bronkhorst EM, Loomans BAC, Huysmans MCDNJM. 12-year survival of composite vs amalgam restorations. Journal of Dental Research.
- Schwendicke F, Samek W, Krois J. Artificial intelligence in dentistry: chances and challenges. Journal of Dental Research.