Can an Inflamed Tooth Nerve Heal on Its Own?
The key difference is whether the nerve inside the tooth can still recover normally once the irritation is removed



Short Answer
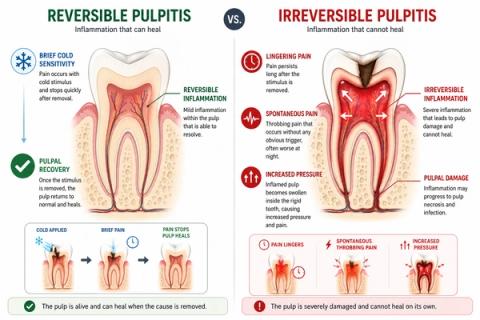
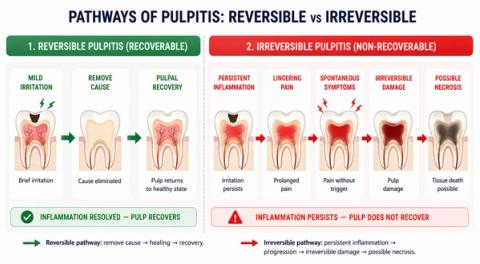
Some cases of tooth nerve inflammation can recover after the cause is removed, while others progress beyond predictable healing and may require root canal treatment. Brief sensitivity is more common in reversible pulpitis, whereas lingering or spontaneous pain is more associated with irreversible disease.
What Happens When the Tooth Nerve Becomes Inflamed?
Pulpitis means inflammation inside the tooth pulp — the soft tissue containing:
- nerves,
- blood vessels,
- and connective tissue.
The important question is:
Can the pulp still recover normally?
Some inflammation remains:
- mild,
- controlled,
- and potentially reversible.
Other cases progress toward:
- persistent inflammation,
- ongoing tissue injury,
- and reduced biologic recovery potential.
When Can an Inflamed Tooth Nerve Still Heal?
In early or mild tooth nerve inflammation:
- inflammation is usually mild or early,
- and the pulp can often recover if the cause is treated promptly.
Common causes include:
- early decay,
- leaking restorations,
- exposed dentin,
- mild irritation,
- or minor crack-related stress.
People commonly notice:
- brief cold sensitivity,
- mild discomfort with sweets,
- occasional chewing or biting sensitivity,
- or pain that stops quickly after the trigger is removed.
People may describe it as:
- “Cold drinks hurt briefly.”
- “Sensitivity disappears quickly.”
- “The tooth reacts but settles fast.”
- “The pain is mild and temporary.”
At this stage:
- the pulp may still maintain normal healing capacity.
When Is Healing Less Likely?
In more advanced tooth nerve inflammation:
- inflammation becomes more severe or prolonged,
- and the pulp is no longer expected to recover predictably.
People may notice:
- lingering cold sensitivity,
- heat sensitivity,
- spontaneous throbbing pain,
- night pain,
- pain that becomes more frequent or intense,
- or chewing and biting discomfort.
People commonly describe:
- “The pain lingers after cold drinks.”
- “Heat causes throbbing pain.”
- “The tooth hurts without warning.”
- “The pain wakes me at night.”
- “Chewing or biting feels uncomfortable.”
As inflammation progresses:
However:symptoms do not always follow a perfectly predictable pattern,and:some teeth with irreversible disease may still present with surprisingly mild symptoms.
Why the Pattern of Symptoms Matters
| Symptom Pattern | What It May Suggest |
|---|---|
| Brief cold sensitivity | Reversible pulpitis |
| Lingering cold pain | Irreversible inflammatory progression |
| Heat sensitivity | More advanced pulpal involvement |
| Spontaneous throbbing pain | Irreversible inflammatory activation |
| Night pain | Advanced pulpal sensitization |
| Pain while chewing or biting | Structural or apical involvement |
| Symptoms improving after treatment | Greater recovery potential |
- symptom behavior,
- vitality response,
- progression pattern,
- radiographic findings,
- and structural conditionrather than relying on one symptom alone.
What This Means
The important question is not simply:
“How much does the tooth hurt?”
but:
“Does the pulp still retain biologic recovery potential?”
Reversible pulpitis suggests:
- inflammatory regulation is still preserved,
- vascular function remains relatively stable,
- and recovery may still occur after eliminating the irritant.
Irreversible pulpitis suggests:
- sustained inflammatory mediator activity,
- altered intrapulpal pressure dynamics,
- progressive neural sensitization,
- and declining healing potential.
Early treatment may help prevent progression from:
- reversible irritation,toward:
- irreversible pulpal compromise,
- necrosis,
- and apical disease.
When to See a Dentist
You should consider evaluation if:
- cold sensitivity lingers,
- heat triggers pain,
- spontaneous pain develops,
- night pain occurs,
- symptoms are increasing over time,
- or chewing or biting discomfort appears.
- thermal response,
- vitality status,
- symptom duration,
- progression pattern,
- radiographic findings,
- and structural integrity—not just pain severity alone.
Early evaluation may improve the chance of preserving pulpal health.
Related Questions
Clinical Perspective
For dental professionalsThis section discusses clinical reasoning and is not intended for self-diagnosis.
Pulpal Inflammation Reversibility – Biologic Recovery vs Irreversible Compromise
Clinical Takeaway
The distinction between reversible and irreversible pulpitis depends on biologic recovery capacity of the pulp rather than symptom intensity alone, requiring interpretation of inflammatory behavior, vitality response, and progression over time.
Interpretation Framework
Pulpitis reversibility represents a biologic continuum rather than an absolute binary state.
Clinical interpretation requires integration of:
- thermal response characteristics,
- spontaneous pain behavior,
- symptom duration,
- progression trajectory,
- structural/restorative status,
- vitality findings,
- and inflammatory persistence.
The key diagnostic question is whether pulpal vascular and neural systems retain predictable recovery potential after elimination of the irritant.
Current interpretation increasingly emphasizes:
- biologic recovery potential,
- temporal inflammatory behavior,
- and progression dynamicsrather than isolated symptom severity.
Current Understanding (Guidelines + Evidence)
Endodontic Perspective (AAE / ESE Aligned)
Reversible pulpitis commonly demonstrates:
- brief stimulus-dependent sensitivity,
- non-lingering cold response,
- absence of spontaneous pain,
- and preserved recovery behavior.
Irreversible pulpitis more commonly demonstrates:
- lingering thermal pain,
- spontaneous episodes,
- nocturnal symptoms,
- heat sensitivity,
- and sustained inflammatory activity.
Important interpretation principles include:
- symptom overlap exists between categories,
- reversibility cannot be determined with absolute certainty histologically from symptoms alone,
- progression is dynamic and patient-specific,
- and symptom behavior over time remains clinically significant.
Pathophysiologic Insight
Reversible states maintain:
- vascular regulation,
- inflammatory containment,
- and adaptive pulpal response.
Irreversible states involve:
- sustained inflammatory mediator activity,
- altered intrapulpal pressure dynamics,
- progressive neural sensitization,
- and declining biologic recovery capacity.
Differential Diagnosis
1. Reversible Pulpitis
Features:
- brief cold sensitivity,
- non-lingering response,
- stimulus-dependent symptoms,
- recoverable inflammatory state.
2. Symptomatic Irreversible Pulpitis
Features:
- lingering thermal response,
- spontaneous throbbing,
- increasing symptom frequency,
- reduced biologic recovery potential.
3. Hyperreactive Dentin Sensitivity
Features:
- sharp brief thermal response,
- no spontaneous pain,
- non-pulpal origin,
- exposed dentin behavior.
4. Cracked Tooth Syndrome
Features:
- intermittent thermal symptoms,
- load-dependent pain,
- structural instability,
- may mimic irreversible pulpitis.
Key Diagnostic Distinctions
| Feature | Reversible pulpitis | Irreversible pulpitis |
|---|---|---|
| Cold response | Brief | Lingering |
| Spontaneous pain | Rare | More common |
| Heat sensitivity | Less characteristic | More characteristic |
| Recovery potential | Preserved | Reduced |
| Progression concern | Lower | Higher |
| Inflammatory persistence | Limited | Sustained |
Common Pitfalls
Common diagnostic errors include:
- assuming all lingering pain guarantees irreversibility,
- over-reliance on single thermal tests,
- ignoring progression trends over time,
- missing crack-related symptom overlap,
- and failure to correlate restorability with structural status.
Pulpal reversibility assessment should always integrate:
- symptom evolution,
- vitality context,
- and restorative prognosis.
Emerging Research Directions
Biologic Reversibility Assessment
Research increasingly focuses on:
- inflammatory biomarker profiling,
- pulpal microcirculation analysis,
- cytokine-mediated recovery prediction,
- and biologic reversibility modeling.
AI-Assisted Interpretation
Emerging systems increasingly evaluate:
- temporal symptom-pattern analysis,
- probabilistic reversibility modeling,
- multimodal vitality integration,
- and progression-risk forecasting.
Advanced Vitality Diagnostics
Current research increasingly explores:
- pulse oximetry,
- laser Doppler flowmetry,
- physiologic pulp monitoring systems,
- and vascular vitality assessment.
AI Potential
Differentiating reversible from irreversible pulpitis represents a progression-interpretation problem where clinical meaning depends on integrating inflammatory behavior, vitality response, and symptom evolution over time.
AI can assist across the clinical workflow:
Interpretation
- Integrating thermal response, symptom duration, spontaneous pain behavior, and progression history
- Identifying clinically meaningful reversibility patterns
Decision Timing
- Supporting monitor versus intervene decisions
- Flagging progression-risk presentations
- Assisting timing-sensitive pulpal management
Patient Communication
- Explaining the difference between recoverable irritation and irreversible damage
- Clarifying why early intervention matters
- Improving understanding of treatment recommendations
Clinical Workflow Support
- Structuring pulpal assessment findings consistently
- Supporting longitudinal symptom interpretation
- Reducing variability in reversibility assessment
Emerging Direction
- AI-assisted pulpal recovery prediction
- Biologic reversibility modeling
- Integration of symptom behavior, vitality testing, and inflammatory analytics
Clinical Relevance
The challenge is not simply identifying pulpal inflammation — it is determining whether the pulp retains biologic recovery potential or whether progression has crossed into irreversible compromise.
AI may eventually help:
- improve interpretation of pulpal reversibility,
- support earlier intervention before irreversible progression,
- reduce variability in treatment decisions,
- and enhance patient communication around pulpal prognosis.
References
- American Association of Endodontists (AAE). Diagnostic Terminology and Clinical Considerations for Endodontic Practice. AAE Clinical Resources.
- Wolters WJ, Duncan HF, Tomson PL, et al. Minimally invasive endodontics: a new diagnostic system for assessing pulpitis and subsequent treatment needs. International Endodontic Journal.
- Baume LJ. Diagnosis of disease of the pulp. Oral Surgery, Oral Medicine, Oral Pathology.
- Hashem D, Mannocci F, Patel S, et al. Clinical and radiographic assessment of the efficacy of different diagnostic tests used for pulpal diagnosis. Journal of Endodontics.
- Trowbridge HO. Pathogenesis of pulpitis resulting from dental caries. Journal of Endodontics.
- Bergenholtz G. Pathogenic mechanisms in pulpal disease. Journal of Endodontics.
- Cooper PR, Holder MJ, Smith AJ. Inflammation and regeneration in the dentin-pulp complex: a double-edged sword. Journal of Endodontics.
- Jafarzadeh H, Abbott PV. Review of pulp sensibility tests. Part I: general information and thermal tests. International Endodontic Journal.
- The Use of Artificial Intelligence in Endodontics - F.C. Setzer, J. Li, A.A. Khan, 2024