Can antibiotics replace root canal treatment?
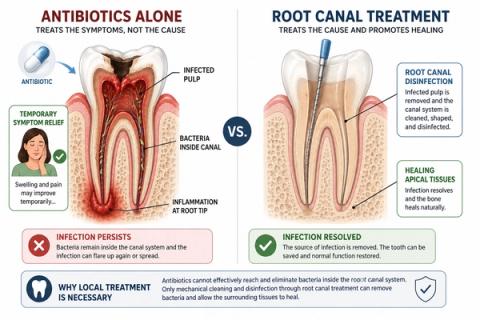
Antibiotics may help control spreading infection temporarily, but they usually cannot eliminate infection trapped inside the root canal system



Short Answer
No, antibiotics usually cannot replace root canal treatment when infection is inside the tooth. Root canal treatment removes infected tissue and disinfects the canal system directly, while antibiotics have limited ability to fully eliminate bacteria inside a non-vital tooth.
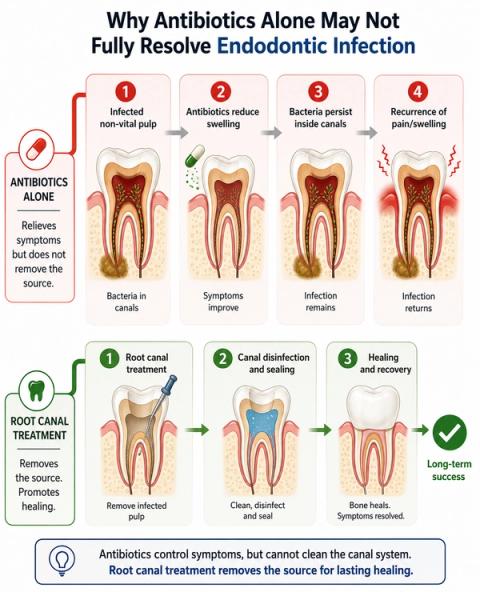
Why Don’t Antibiotics Alone Usually Fix Tooth Infection?
When infection develops inside a tooth:
- bacteria often become trapped within the root canal system,
- and blood supply inside the pulp may become severely reduced or absent.
Because of this:
- antibiotics may not reach the infection effectively enough to eliminate it completely.
People often assume:
- antibiotics will “kill the infection.”
However:the infected tissue and bacteria inside the tooth usually remain unless the canal system is cleaned and disinfected directly.
What Can Antibiotics Help With?
Antibiotics may still help:
- reduce swelling,
- limit spreading infection,
- control systemic involvement,
- and reduce risk of wider tissue spread.
They are especially important when:
- swelling is spreading,
- fever develops,
- facial swelling occurs,
- cellulitis is present,
- or systemic involvement increases.
However:antibiotics alone usually do not:
- remove infected pulp tissue,
- disinfect the root canal system predictably,
- or permanently eliminate the source of infection.
What Does Root Canal Treatment Actually Do?
Root canal treatment aims to:
- remove infected pulp tissue,
- disinfect the canal system,
- reduce bacterial load directly,
- and preserve the tooth structure. [Siqueira JF Jr & Rôças IN]
Without local treatment:
- symptoms may return,
- infection may continue progressing,
- swelling or abscess formation may recur,
- and structural damage may worsen over time.
This is why:
- definitive treatment usually requires:
- root canal treatment,
- drainage,
- extraction,
- or another form of local source control.
Why the Pattern of Symptoms Matters
| Symptom Pattern | What It May Suggest |
|---|---|
| Severe tooth pain without swelling | Localized pulpal disease |
| Swelling or facial enlargement | Infection spreading beyond the tooth |
| Temporary improvement after antibiotics | Symptom suppression without source removal |
| Recurring swelling | Persistent canal infection |
| Pain while chewing or biting | Apical inflammatory involvement |
| Fever or systemic illness | More urgent infection spread risk |
Dentists evaluate:
- swelling extent,
- systemic signs,
- pulpal vitality,
- apical involvement,
- and infection spread riskrather than prescribing antibiotics based on pain alone.
What This Means
The important question is not simply:
“Did the antibiotics reduce the pain?”
but:
“Was the source of infection actually removed?”
A non-vital infected tooth often behaves differently from infections elsewhere in the body because:
- vascular supply becomes compromised,
- bacteria organize within canal biofilms,
- and microbial control becomes difficult without direct canal debridement.
This means:
- symptoms may improve temporarily,while:
- underlying infection persists silently inside the tooth.
Delaying definitive treatment may increase:
- infection progression,
- swelling recurrence,
- structural weakening,
- and long-term prognosis uncertainty.
When to See a Dentist
You should consider evaluation if:
- swelling develops,
- pain becomes severe or spontaneous,
- symptoms return after antibiotics,
- chewing or biting becomes difficult,
- drainage or bad taste occurs,
- or fever or facial swelling develops.
- infection extent,
- pulpal vitality,
- swelling pattern,
- apical involvement,
- and systemic risk—not just pain intensity alone.
Early evaluation may help prevent progression toward more extensive infection.
Related Questions
Clinical Perspective
For dental professionalsThis section discusses clinical reasoning and is not intended for self-diagnosis.
Antibiotics in Endodontic Infection – Systemic Support vs Local Disease Control
Clinical Takeaway
Antibiotics are adjunctive rather than definitive therapy for most endodontic infections because:
- the primary disease source is localized within the root canal system,
- and predictable resolution requires mechanical and chemical debridement.
Interpretation Framework
Endodontic infection management should be interpreted primarily as a:
- local microbial control problemrather than solely:
- a systemic infectious process.
Clinical assessment requires integration of:
- pulpal vitality status,
- apical involvement,
- swelling extent,
- systemic signs,
- drainage status,
- immune competence,
- and local source-control feasibility.
The key distinction is whether:
“The infection remains localized within the canal system or has progressed into spreading systemic involvement.”
Current interpretation increasingly emphasizes:
- source-control prioritization,
- antimicrobial stewardship,
- and progression-risk assessment.
Current Understanding (Guidelines + Evidence)
Endodontic Perspective (AAE / ESE Aligned)
Antibiotics are generally not indicated for:
- symptomatic irreversible pulpitis alone,
- localized endodontic pain without systemic involvement,
- or cases where local debridement can adequately control infection.
Antibiotics may be indicated when:
- diffuse swelling is present,
- systemic symptoms occur,
- cellulitis develops,
- infection spread risk increases,
- or host compromise exists.
Important interpretation principles include:
- antibiotics alone rarely eliminate intraradicular infection,
- source control remains central to treatment success,
- overprescribing contributes to antimicrobial resistance,
- and symptom suppression does not equal biologic resolution.
Biologic Insight
Necrotic canal systems often demonstrate:
- severely limited vascular supply,
- persistent intraradicular biofilms,
- and reduced antibiotic penetration.
Bacterial biofilms within the canal system are difficult to eliminate through systemic therapy alone.
Mechanical disruption and irrigation therefore remain essential for:
- microbial reduction,
- biofilm disruption,
- and long-term healing predictability.
Differential Diagnosis
1. Symptomatic Irreversible Pulpitis
Features:
- antibiotics generally not indicated,
- local endodontic treatment preferred,
- limited benefit from systemic therapy alone.
2. Localized Acute Apical Abscess
Features:
- drainage and local treatment prioritized,
- adjunctive antibiotics selectively considered.
3. Diffuse Spreading Infection
Features:
- systemic antibiotics commonly indicated adjunctively,
- urgent source control required,
- increased systemic spread risk.
4. Persistent Endodontic Infection
Features:
- retreatment or surgical management may be required,
- antibiotics alone insufficient for predictable resolution.
Key Diagnostic Distinctions
| Feature | Antibiotics alone | Root canal treatment |
|---|---|---|
| Removes infected pulp | No | Yes |
| Eliminates canal bacteria predictably | Limited | More effective |
| Controls local source | Limited | Directly targeted |
| Useful in systemic spread | Adjunctive role | Still necessary |
| Long-term infection control | Unreliable alone | More predictable |
Common Pitfalls
Common diagnostic errors include:
- prescribing antibiotics without local source control,
- treating pain alone rather than infection biology,
- assuming temporary symptom improvement equals resolution,
- overusing antibiotics in irreversible pulpitis,
- and delaying definitive treatment because symptoms transiently improve.
Infection management should always integrate:
- biologic source control,
- systemic spread assessment,
- and long-term prognosis.
Emerging Research Directions
Biofilm Disruption Technologies
Research increasingly focuses on:
- enhanced irrigant activation,
- antimicrobial nanoparticle systems,
- targeted intracanal therapeutics,
- and advanced biofilm-disruption strategies.
AI-Assisted Infection Assessment
Emerging systems increasingly evaluate:
- severity-risk stratification,
- systemic spread prediction,
- treatment urgency modeling,
- and multimodal infection interpretation.
Antimicrobial Stewardship
Current research increasingly explores:
- optimized prescribing analytics,
- resistance-risk prediction,
- precision infection management,
- and decision-support stewardship systems.
AI Potential
Determining when antibiotics are appropriate represents a:
- local-versus-systemic infection interpretation problemwhere clinical meaning depends on integrating:
- biologic spread,
- source-control needs,
- and host response.
AI can assist across the clinical workflow:
Interpretation
- Integrating swelling pattern, systemic findings, vitality status, and imaging
- Identifying clinically meaningful spread-risk patterns
Decision Timing
- Supporting urgency assessment
- Flagging cases requiring adjunctive antibiotic therapy
- Assisting source-control prioritization
Patient Communication
- Explaining why antibiotics alone may not eliminate tooth infection
- Clarifying the difference between symptom suppression and infection removal
- Improving understanding of definitive treatment needs
Clinical Workflow Support
- Structuring infection-severity assessment
- Supporting antimicrobial stewardship consistency
- Reducing variability in antibiotic prescribing decisions
Emerging Direction
- AI-assisted endodontic infection stratification
- Predictive spread-risk modeling
- Integrated antimicrobial stewardship analytics
Clinical Relevance
The challenge is not simply prescribing antibiotics — it is determining whether the infection can be predictably controlled without:
- definitive local source removal,
- canal disinfection,
- and biologic resolution of the infected tooth.
AI may eventually help:
- improve infection-severity interpretation,
- support more appropriate antibiotic utilization,
- reduce unnecessary prescribing,
- and enhance patient understanding of definitive endodontic treatment needs.
References
- American Association of Endodontists (AAE). AAE Guidance on the Use of Systemic Antibiotics in Endodontics. AAE Clinical Resources.
- European Society of Endodontology (ESE). Position statement: the use of antibiotics in endodontics. International Endodontic Journal.
- Segura-Egea JJ, Gould K, Şen BH, et al. Antibiotics in Endodontics: a review. International Endodontic Journal.
- Fouad AF, Rivera EM, Walton RE. Penicillin as a supplement in resolving the localized acute apical abscess. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology.
- Siqueira JF Jr, Rôças IN. Optimising single-visit disinfection with supplementary approaches: a quest for predictability. Australian Endodontic Journal.
- Mohammadi Z, Abbott PV. On the local applications of antibiotics and antibiotic-based agents in endodontics and dental traumatology. International Endodontic Journal.
- Cope AL, Francis NA, Wood F, Chestnutt IG. Antibiotic prescribing in UK general dental practice: a cross-sectional study. Community Dentistry and Oral Epidemiology.
- Schwendicke F, Samek W, Krois J. Artificial intelligence in dentistry: chances and challenges. Journal of Dental Research.