Root canal vs extraction – which is better?
The better option is usually the one that provides the most predictable long-term function, stability, and health for that specific tooth and patient.



Short Answer
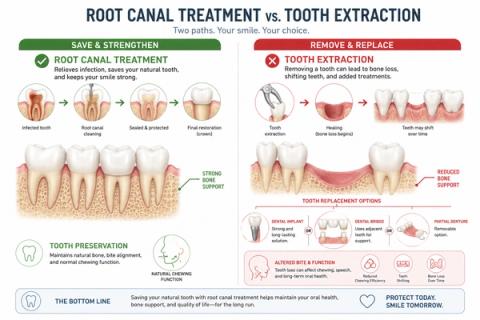
Root canal treatment is often preferred when the tooth can still be predictably restored and maintained, because preserving the natural tooth helps maintain chewing and biting function, jaw stability, and surrounding support. Extraction may be considered when the tooth is severely damaged, structurally non-restorable, or has a poor long-term prognosis despite treatment.
Why Do Dentists Sometimes Recommend Root Canal Instead of Extraction?
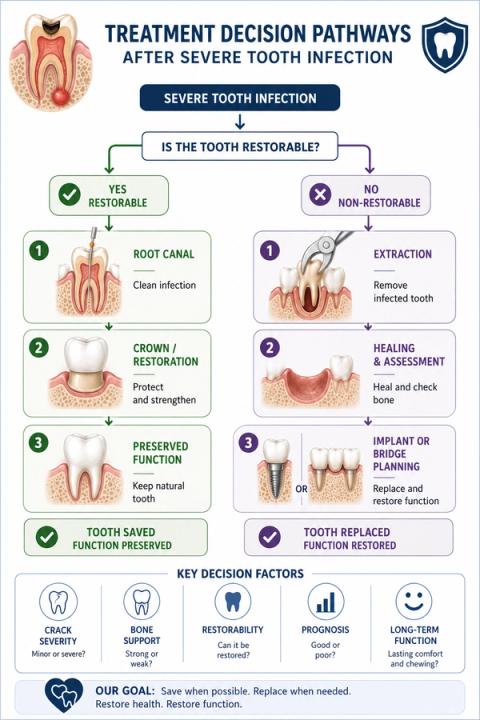
When a tooth becomes severely infected, inflamed, or damaged, treatment decisions often involve two broad options:
- preserve the tooth,or:
- remove the tooth completely.
Many people assume:
- extraction is automatically the easier or better option.
However:preserving the natural tooth is often preferred when long-term restoration remains predictable. [Ng YL et al.]
This is because the natural tooth helps:
- maintain chewing and biting mechanics,
- stabilize nearby teeth,
- preserve jawbone stimulation,
- and maintain normal bite alignment.
What Does Root Canal Treatment Aim to Do?
Root canal treatment aims to:
- remove infection from inside the tooth,
- preserve the natural tooth structure,
- maintain chewing and biting function,
- and help maintain long-term oral stability.
It may be preferred when:
- the tooth is structurally restorable,
- surrounding bone support is adequate,
- cracks are manageable,
- and long-term function is achievable.
Preserving the natural tooth often helps:
- maintain bite stability,
- reduce shifting of nearby teeth,
- preserve physiologic chewing mechanics,
- and maintain normal proprioceptive feedback through the periodontal ligament.
When Is Extraction Sometimes the Better Option?
Extraction removes the tooth completely.
It may be considered when:
- the tooth is severely fractured,
- structural damage is extensive,
- periodontal support is poor,
- restorability is extremely limited,
- or long-term prognosis remains unfavorable despite treatment.
After extraction:
- replacement options such as implants, bridges, or removable prostheses may be discussed depending on the situation.
However:extraction is not automatically the “simpler” long-term solution,and:replacement teeth do not biologically behave exactly like natural teeth.
Why the Long-Term Prognosis Matters
| Clinical Factor | Root Canal Often Favored | Extraction More Likely Favored |
|---|---|---|
| Remaining tooth structure | Adequate/restorable | Severely compromised |
| Fracture status | Stable/manageable | Vertical/non-restorable fracture |
| Bone and gum support | Maintainable | Advanced loss |
| Long-term restorability | Predictable | Poor/unpredictable |
| Strategic tooth importance | High | Limited |
| Functional prognosis | Favorable | Unfavorable |
- restorability,
- fracture status,
- periodontal support,
- infection extent,
- and long-term prognosisrather than focusing only on pain or short-term cost.
What This Means
The important question is not simply:
“Can the tooth be treated?”
but:
“Can the tooth function predictably long term?”
Some severely damaged teeth can still function successfully for many years after:
- root canal treatment,
- proper restoration,
- and long-term maintenance.
Other teeth may have:
- structural instability,
- advanced fracture patterns,
- or severe support lossthat makes long-term preservation biologically unrealistic.
Modern dentistry increasingly emphasizes:
- prognosis-based decision-making,rather than:
- automatic extraction or automatic preservation.
When to See a Dentist
You should consider evaluation if:
- severe tooth pain develops,
- swelling or infection appears,
- a tooth fractures,
- chewing or biting becomes difficult,
- a dentist identifies deep structural damage,
- or previous treatment has failed repeatedly.
- restorability,
- fracture status,
- bone support,
- infection extent,
- bite function,
- and long-term prognosis—not just whether the tooth currently hurts.
Early evaluation may improve the chances of preserving the natural tooth when appropriate.
Related Questions
Clinical Perspective
For dental professionalsThis section discusses clinical reasoning and is not intended for self-diagnosis.
Tooth Preservation vs Extraction – Biologic and Restorative Decision-Making
Clinical Takeaway
The decision between root canal treatment and extraction depends primarily on:
- long-term restorability,
- structural prognosis,
- periodontal support,
- and functional predictabilityrather than symptom severity alone.
Interpretation Framework
Root canal versus extraction represents a:
- prognosis-based,
- biologic,
- structural,
- and restorative decision problem.
Clinical assessment requires integration of:
- restorability,
- fracture status,
- ferrule adequacy,
- periodontal support,
- strategic tooth value,
- endodontic prognosis,
- occlusal considerations,
- and patient-specific maintenance capacity.
The key question is not whether:
“The tooth can technically undergo treatment,”
but whether:
“Predictable long-term biologic and functional stability can realistically be maintained.”
Current interpretation increasingly emphasizes:
- prognosis-oriented preservation,
- structural fatigue assessment,
- and long-term functional predictabilityrather than procedural simplicity alone.
Current Understanding (Guidelines + Evidence)
Endodontic / Restorative Perspective (AAE / ESE Aligned)
Root canal treatment is commonly favored when:
- adequate remaining tooth structure exists,
- periodontal support is maintainable,
- long-term restoration is feasible,
- and structural prognosis remains acceptable.
Extraction may be favored when:
- vertical root fracture is present,
- restorability is severely compromised,
- periodontal destruction is advanced,
- recurrent structural failure is likely,
- or strategic prognosis is poor.
Important interpretation principles include:
- preservation of the natural tooth remains biologically advantageous when prognosis is favorable,
- extraction initiates secondary restorative and maintenance decisions,
- implant replacement and natural-tooth preservation are not biologically identical pathways,
- and prognosis — not procedural convenience — should guide treatment selection.
Biomechanical Insight
Preserved periodontal ligament contributes to:
- proprioception,
- physiologic load distribution,
- and adaptive occlusal feedback.
Extraction alters:
- local biomechanics,
- bone remodeling dynamics,
- and functional loading patterns.
Structural fatigue behavior and ferrule adequacy critically influence:
- fracture resistance,
- restorative predictability,
- and long-term survival.
Differential Diagnosis
1. Restorable tooth with irreversible pulpitis
- favorable endodontic candidat
- preservation generally preferred
2. Tooth with vertical root fracture
- extraction commonly indicated
- poor long-term structural prognosis
3. Advanced periodontal-endodontic compromise
- prognosis dependent on attachment support and restorability
4. Severely broken-down tooth
- ferrule/restorative limitations
- questionable long-term function despite successful endodontics
Key Diagnostic Distinctions
| Factor | Root canal favored | Extraction favored |
|---|---|---|
| Restorability | Adequate | Severely compromised |
| Fracture status | Repairable/stable | Vertical/non-restorable |
| Periodontal support | Maintainable | Poor/advanced loss |
| Strategic value | High | Limited |
| Long-term prognosis | Favorable | Unfavorable |
| Ferrule adequacy | Achievable | Unachievable |
Common Pitfalls
Common diagnostic errors include:
- initiating endodontic treatment without restorability analysis,
- overestimating implant superiority universally,
- ignoring structural fatigue and ferrule limitations,
- failing to integrate periodontal prognosis,
- and making extraction decisions primarily from acute symptoms.
Preservation decisions should always integrate:
- biologic prognosis,
- restorative feasibility,
- and long-term functional predictability.
Emerging Research Directions
Prognostic Modeling
Research increasingly focuses on:
- long-term restorability analytics,
- structural fatigue prediction,
- survival-outcome integration,
- and biologic prognosis modeling.
AI-Assisted Treatment Planning
Emerging systems increasingly evaluate:
- restorability prediction,
- fracture-risk modeling,
- multimodal prognosis estimation,
- and long-term survival analytics.
Biomechanical Analytics
Current research increasingly explores:
- occlusal stress simulation,
- structural load-distribution modeling,
- ferrule optimization,
- and restoration longevity prediction.
AI Potential
Root canal versus extraction decisions represent complex prognosis-interpretation problems where clinical meaning emerges from integrating:
- structural,
- biologic,
- restorative,
- periodontal,
- and functional variables.
AI can assist across the clinical workflow:
Interpretation
- Integrating restorability, periodontal support, imaging, and fracture-risk findings
- Identifying clinically meaningful long-term prognosis patterns
Decision Timing
- Supporting preservation versus extraction planning
- Flagging structural failure-risk scenarios
- Assisting prognosis-oriented sequencing decisions
Patient Communication
- Explaining why preserving the natural tooth is often preferred when feasible
- Clarifying long-term implications of extraction and replacement
- Improving understanding of prognosis-based decision-making
Clinical Workflow Support
- Structuring restorability assessment consistently
- Supporting longitudinal prognosis tracking
- Reducing variability in treatment-planning interpretation
Emerging Direction
- AI-assisted restorability prediction
- Multimodal prognosis modeling integrating imaging and structural analytics
- Predictive long-term survival assessment for endodontically treated teeth
Clinical Relevance
The challenge is not simply deciding whether to perform root canal treatment or extraction — it is determining which pathway offers the most predictable:
- long-term biologic stability,
- functional performance,
- and restorative prognosisfor the specific tooth and patient.
AI may eventually help:
- improve prognosis-oriented decision-making,
- support earlier recognition of non-restorable conditions,
- reduce variability in treatment planning,
- and enhance patient communication regarding long-term outcomes.
References
- American Association of Endodontists (AAE). Treatment Options for the Compromised Tooth: A Decision Guide. AAE Clinical Resources.
- European Society of Endodontology (ESE). Quality guidelines for endodontic treatment. International Endodontic Journal.
- Ng YL, Mann V, Gulabivala K. Tooth survival following non-surgical root canal treatment: a systematic review of the literature. International Endodontic Journal.
- Torabinejad M, Anderson P, Bader J, et al. Outcomes of root canal treatment and restoration, implant-supported single crowns, fixed partial dentures, and extraction without replacement: a systematic review. Journal of Prosthetic Dentistry.
- Sorensen JA, Engelman MJ. Ferrule design and fracture resistance of endodontically treated teeth. Journal of Prosthetic Dentistry.
- Fuss Z, Lustig J, Tamse A. Prevalence of vertical root fractures in extracted endodontically treated teeth. International Endodontic Journal.
- Avila G, Galindo-Moreno P, Soehren S, et al. A novel decision-making process for tooth retention or extraction. Journal of Periodontology.
- Schwendicke F, Samek W, Krois J. Artificial intelligence in dentistry: chances and challenges. Journal of Dental Research.