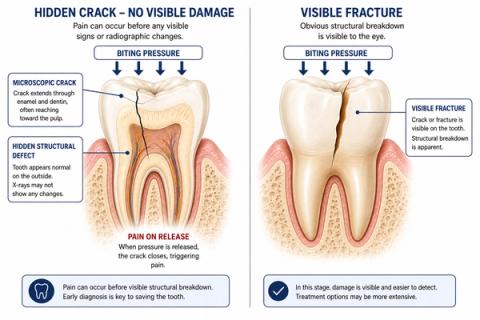
Can a cracked tooth cause pain without visible damage?
Cracks in teeth are often microscopic or hidden — the pain may appear long before the damage becomes visibly obvious



Short Answer
Yes, a cracked tooth can cause pain even when no visible damage appears on the tooth or X-ray. Small cracks may alter how force travels through the tooth, triggering pain during chewing, biting, release of pressure, or temperature changes before the crack becomes clinically visible. Pain from hidden cracks is often intermittent and difficult to reproduce consistently, which is why early crack-related pain is commonly missed.
Can a Tooth Crack Without Looking Broken?
Yes.
A tooth does not need to visibly break to develop crack-related pain.
- form inside the tooth structure,
- remain invisible externally,
- or fail to appear clearly on routine X-rays.
Even when the tooth looks normal, the crack may still change how pressure moves through the tooth during chewing or biting.
People commonly describe it as:
- “Sharp pain when I bite down.”
- “Pain when I release pressure.”
- “The tooth hurts sometimes but looks normal.”
- “Cold sensitivity comes and goes.”
- “The pain is difficult to reproduce consistently.”
- “One tooth feels strange while chewing.”
This often causes confusion because:
- symptoms may come and go,
- the tooth may appear intact,
- and imaging may initially look normal.
Why Can Hidden Cracks Cause Pain?
A cracked tooth changes how stress travels through the enamel and dentin.
- pressure may cause tiny movements inside the crack,
- the tooth may flex abnormally,
- and surrounding tissues or the nerve inside the tooth may become irritated.
Pain may occur:
- during pressure,
- after releasing pressure,
- or with temperature changes.
In some cases:
- cracks irritate the nerve inside the tooth,while in others:
- the pain comes mainly from mechanical stress during biting or chewing.
- inflammation,
- lingering sensitivity,
- or root-area irritationmay also begin developing.
Why the Pattern of Pain Matters
| Pain Pattern | What It May Suggest |
|---|---|
| Sharp pain while biting | Possible structural crack |
| Pain on release of pressure | More characteristic of cracked teeth |
| Intermittent chewing pain | Early crack behavior |
| Cold sensitivity with biting pain | Crack-related pulpal irritation |
| Tooth looks normal but hurts | Hidden structural instability |
| Symptoms difficult to reproduce | Occult crack presentation |
- load-response behavior,
- release pain,
- thermal sensitivity,
- symptom timing,
- and structural findingsrather than relying only on visible damage or X-rays.

What This Means
Crack-related pain is often a functional problem before it becomes a visible structural problem.
This means:
- the tooth may hurt before the crack becomes visible,
- symptoms may appear long before radiographic findings develop,
- and pain patterns may fluctuate over time.
Normal X-rays do not reliably exclude clinically important cracks.
Early crack-related symptoms may still indicate:
- progressing structural weakness,
- pulpal irritation,
- or increasing fracture risk.
- prevent crack progression,
- preserve more tooth structure,
- and reduce the risk of more extensive treatment later.
When to See a Dentist
You should consider evaluation if:
- sharp pain occurs during chewing or biting,
- pain appears on release of biting pressure,
- symptoms are intermittent but recurring,
- cold sensitivity develops,
- one tooth repeatedly feels uncomfortable despite looking normal,
- or chewing becomes difficult on one side.
A dentist evaluates:
- bite response,
- release pain,
- crack-line detection,
- thermal response,
- and structural integrity—not just radiographic appearance alone.
Related Questions
Clinical Perspective
For dental professionalsThis section discusses clinical reasoning and is not intended for self-diagnosis.
Occult Cracked Tooth Syndrome – Structural Pain Without Radiographic Visibility
Clinical Takeaway
Cracked teeth frequently produce clinically significant symptoms before visible structural or radiographic evidence develops; diagnosis depends primarily on interpretation of load-response behavior and symptom patterns.
Interpretation Framework
Occult crack pathology represents a structural instability phenomenon where force-distribution changes precede obvious morphologic breakdown.
Interpretation requires integrating:
- biting and release pain behavior,
- thermal sensitivity,
- occlusal loading response,
- restoration status,
- crack propagation risk,
- and structural testing findings.
The absence of visible radiographic findings does not meaningfully exclude clinically significant crack-related pathology.
Current interpretation increasingly emphasizes:
- functional load behavior,
- progression risk,
- and symptom reproducibility under controlled loadingrather than radiographic visibility alone.
Current Understanding (Guidelines + Evidence)
Endodontic / Restorative Perspective (AAE Aligned)
Cracked teeth may:
- remain radiographically occult,
- present intermittently,
- produce variable thermal symptoms,
- and mimic pulpal or apical disease.
Pain patterns commonly include:
- sharp pain on release,
- load-triggered discomfort,
- intermittent localization difficulty,
- and cold sensitivity.
Important interpretation principles include:
- cracks are frequently diagnosed clinically rather than radiographically,
- symptom reproducibility under controlled loading is highly valuable,
- progression risk depends on force distribution and crack depth,
- and pulpal involvement may occur secondarily as crack propagation advances.
Biomechanical Insight
Crack propagation alters stress distribution through enamel and dentin.
Separation forces during release may intensify nociceptive activation, while repeated cyclic loading contributes to progressive structural fatigue.
Occult cracks therefore represent:
- both a structural,and:
- a biomechanical progression phenomenon.
Differential Diagnosis
1. Cracked Tooth Syndrome
Features:
- pain on biting or release,
- intermittent symptoms,
- variable thermal response,
- minimal radiographic findings.
2. Symptomatic Irreversible Pulpitis
Features:
- lingering thermal pain,
- spontaneous symptoms,
- less mechanically specific presentation.
3. Symptomatic Apical Periodontitis
Features:
- percussion sensitivity,
- pressure discomfort,
- less characteristic release pain.
4. Occlusal Trauma
Features:
- diffuse load-related discomfort,
- generalized soreness,
- functional overload pattern.
Key Diagnostic Distinctions
| Feature | Cracked tooth | Pulpal/apical pathology |
|---|---|---|
| Pain on release | More characteristic | Less characteristic |
| Radiographic findings | Often absent | May develop |
| Symptom pattern | Intermittent/load-dependent | More inflammatory/progressive |
| Localization | Sharp/variable | Often diffuse |
| Thermal sensitivity | Variable | More consistently inflammatory |
| Reproducibility | Controlled loading useful | Less mechanically dependent |
Common Pitfalls
Common diagnostic errors include:
- assuming normal radiographs exclude cracks,
- overdiagnosing endodontic disease,
- missing incomplete or vertical crack patterns,
- failure to reproduce symptoms under controlled loading,
- and ignoring occlusal contribution to crack propagation.
Occult structural instability is commonly underdiagnosed because:
- symptoms fluctuate,
- imaging sensitivity is limited,
- and visible morphologic change may lag behind functional pathology.
Emerging Research Directions
Advanced Crack Detection
Research increasingly focuses on:
- AI-assisted imaging analysis,
- optical coherence tomography,
- near-infrared transillumination,
- and high-resolution CBCT interpretation.
Biomechanical Modeling
Emerging work increasingly evaluates:
- crack-propagation stress analysis,
- load-distribution simulation,
- and structural fatigue prediction.
Current direction emphasizes:
- progression-risk modeling,
- and earlier identification of structurally vulnerable teeth.
Diagnostic Integration
Research increasingly supports:
- combining mechanical testing with imaging,
- multimodal symptom analytics,
- and probabilistic structural-risk interpretation.
AI Potential
Occult cracked teeth represent a structural interpretation problem where clinically meaningful instability may exist before obvious visual evidence appears.
AI can assist across the clinical workflow:
Interpretation
- Integrating load-response behavior, thermal sensitivity, and imaging findings
- Identifying clinically meaningful crack-related patterns
Decision Timing
- Supporting monitor vs intervene decisions
- Flagging progression-risk patterns
- Assisting restorative versus endodontic treatment planning
Patient Communication
- Explaining how cracks may exist without visible damage
- Clarifying why symptoms can fluctuate
- Improving understanding of progression risk and treatment rationale
Clinical Workflow Support
- Structuring crack-related findings systematically
- Supporting consistent load-response interpretation
- Reducing variability in crack diagnosis
Emerging Direction
- AI-assisted occult crack detection
- Multimodal structural-risk modeling
- Predictive crack-propagation analytics integrating symptoms and imaging
Clinical Relevance
The challenge is not simply detecting visible fractures — it is recognizing early structural instability before progression leads to pulpal involvement or catastrophic tooth failure.
AI may eventually help:
- improve early crack interpretation,
- support earlier intervention decisions,
- reduce misdiagnosis of occult structural disease,
- and enhance patient communication around invisible pathology.
References
- American Association of Endodontists (AAE). Cracked Teeth: Clinical Diagnosis and Treatment Recommendations. AAE Clinical Resources.
- Cameron CE. Cracked-tooth syndrome. Journal of the American Dental Association.
- Rivera EM, Walton RE. Cracking the cracked tooth code: detection and treatment of various longitudinal tooth fractures. Endodontic Topics.
- Krell KV, Rivera EM. A six-year evaluation of cracked teeth diagnosed with reversible pulpitis: treatment and prognosis. Journal of Endodontics.
- Hiatt WH. Incomplete crown-root fracture in pulpal-periodontal disease. Journal of Periodontology.
- Banerji S, Mehta SB, Millar BJ. Cracked tooth syndrome. Part 1: aetiology and diagnosis. British Dental Journal.
- Lubisich EB, Hilton TJ, Ferracane J. Cracked teeth: a review of the literature. Journal of Esthetic and Restorative Dentistry.
- Yu M, Li J, Liu S, et al. Diagnosis of cracked tooth: Clinical status and research progress. Japanese Dental Science Review. .