Can tooth pain go away without treatment?
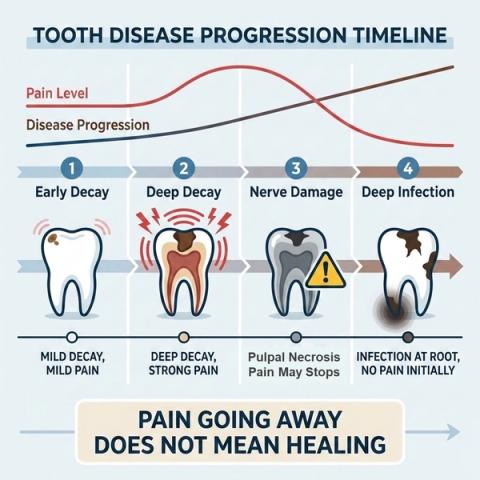
Tooth pain going away doesn’t always mean the problem is gone — it may mean the tooth is no longer responding



Short Answer
Yes, tooth pain can go away without treatment — but this does not always mean the tooth has healed. In some cases, pain disappears because the nerve inside the tooth loses vitality and stops responding, even while infection or disease continues progressing underneath. Dentists evaluate changes in pain patterns carefully because disappearing symptoms can sometimes indicate worsening disease rather than recovery.
Can Tooth Pain Really Disappear on Its Own?
Yes — tooth pain can temporarily reduce or disappear without treatment.
People commonly describe it as:
- “The tooth stopped hurting suddenly.”
- “The pain disappeared after a few days.”
- “My tooth feels normal again.”
- “Cold sensitivity went away.”
- “The tooth used to hurt badly, but now it doesn’t.”
This sometimes happens because:
- irritation temporarily settles,
- the tooth adapts to the stimulus,
- or the nerve inside the tooth loses its ability to respond.
The important point:absence of pain does not always mean absence of disease.
Why Can Tooth Pain Disappear?
The nerve inside the tooth (pulp) reacts to irritation, inflammation, and infection.
In early stages:
- the tooth may feel sensitive to cold,
- chewing or biting may hurt,
- and pain may come and go.
As inflammation progresses, the nerve may gradually lose vitality.
When this happens:
- cold sensitivity may disappear,
- pain may suddenly reduce,
- or the tooth may stop responding completely.
In some cases, people assume:
“The pain went away, so the tooth healed.”
But the underlying problem — such as decay, infection, or a crack — may still continue progressing.
Why the Pattern of Pain Matters
| Pain Pattern | What It May Suggest |
|---|---|
| Pain disappears after mild irritation settles | Temporary recovery |
| Cold sensitivity suddenly disappears | Possible nerve damage |
| Severe pain followed by silence | Possible pulpal necrosis |
| Pain replaced by pressure or swelling | Spreading infection |
| Tooth feels “heavy” or different | Inflammation around the root |
| No pain but darkening tooth | Loss of vitality |
Dentists evaluate:
- previous pain history,
- changes in sensitivity,
- response to testing,
- and progression over timerather than relying only on current symptoms.
What This Means
A tooth becoming painless does not automatically mean the tooth is healthy.
Sometimes symptom resolution may reflect:
- reduced inflammation,
- temporary adaptation,
- or progression toward nerve death inside the tooth.
Even without pain, the tooth may still develop:
- infection near the root,
- swelling,
- biting discomfort,
- or bone changes over time.
Early evaluation can help determine whether the tooth is:
- healing,
- stable,
- or progressing silently toward more advanced disease.
When to See a Dentist
You should consider evaluation if:
- pain suddenly disappears after being persistent,
- cold sensitivity stops unexpectedly,
- the tooth feels different or “heavy,”
- swelling develops,
- chewing or biting becomes uncomfortable,
- or the tooth previously had repeated pain episodes.
A dentist evaluates:
- history of symptoms,
- response to thermal testing,
- tooth structure,
- and signs of underlying infection—not just whether pain is currently present.
Related Questions
Clinical Perspective
For dental professionalsThis section discusses clinical reasoning and is not intended for self-diagnosis.
Pain Resolution vs Pulpal Necrosis
Clinical Takeaway
Disappearance of pain is not a reliable indicator of biologic resolution. Interpretation requires integration of:
- prior symptom history,
- vitality testing,
- radiographic findings,
- and progression patternto distinguish recovery from pulpal necrosis.
Interpretation Framework
Resolution of pain does not necessarily equate to resolution of pathology.
Symptom disappearance may reflect:
- reduction of inflammatory activity,
- neural adaptation,
- vascular compromise,
- or pulpal necrosis with loss of sensory response.
Clinical interpretation therefore requires distinguishing:
- symptom resolution,from
- disease progression.
Current understanding increasingly emphasizes longitudinal symptom behavior and vitality assessment rather than pain presence alone.
Current Understanding (Guidelines + Evidence)
Endodontic Perspective (ESE / AAE Aligned)
Diagnosis should integrate:
- prior pain episodes,
- thermal/electric vitality testing,
- radiographic findings,
- and structural assessment.
Key implication:absence of pain is not a reliable indicator of pulpal health.
Pulpal Progression Insight
Typical biologic progression may involve:
- reversible pulpitis,
- irreversible pulpitis,
- pulpal necrosis,
- followed by apical involvement.
Clinical progression may therefore appear as:
| Stage | Typical Symptom Pattern |
|---|---|
| Reversible pulpitis | Short stimulus-dependent pain |
| Irreversible pulpitis | Increasing spontaneous or lingering pain |
| Necrosis | Reduced or absent sensory response |
| Chronic apical disease | Often asymptomatic until exacerbation |
Critical point:loss of pain may reflect loss of vitality rather than healing.
Differential Diagnosis
1. Resolved Reversible Pulpitis
Features:
- pain subsides after irritant removal,
- tooth remains vital,
- stable symptom course,
- no progressive pathology.
2. Pulpal Necrosis (Post-Symptomatic Phase)
Features:
- prior pain history,
- disappearance of thermal sensitivity,
- absent vitality response,
- possible asymptomatic progression apically.
3. Chronic Apical Periodontitis
Features:
- frequently asymptomatic,
- possible biting discomfort,
- radiographic apical changes,
- later swelling or sinus tract development.
Key Diagnostic Distinctions
| Feature | Healing | Necrosis |
|---|---|---|
| Pain disappearance | Gradual, with reduced triggers | Often follows intense pain |
| Thermal response | Present | Absent |
| Vitality testing | Positive | Negative |
| Radiographic signs | Absent | May develop apically |
| Clinical course | Stable | Progressive |
Common Pitfalls
Common diagnostic errors include:
- assuming pain resolution equals healing,
- failure to perform vitality testing,
- underestimating asymptomatic necrosis,
- and delayed intervention due to false reassurance.
Symptom absence may mask ongoing biologic progression.
Emerging Research Directions
Pulp Vitality Assessment
Research increasingly focuses on:
- laser Doppler flowmetry,
- pulse oximetry,
- and AI based-objective pulp vitality assessmentrather than relying solely on sensory response testing.
Disease Progression Modeling
Emerging work aims to better characterize:
- inflammation-to-necrosis transition,
- asymptomatic progression patterns,
- and predictors of vitality loss.
Current direction increasingly emphasizes biologic status rather than symptom presence alone.
AI Potential
Loss of pain represents a critical interpretation point, where symptom resolution may reflect either recovery or progression before definitive clinical findings become obvious.
AI can assist across the clinical workflow:
Interpretation
- Analyzing longitudinal symptom history(e.g., intermittent pain → sudden resolution)
- Identifying patterns suggestive of necrosis progression
Decision Timing
- Supporting decisions in ambiguous scenarios(monitor vs intervene)
- Flagging risk of underlying necrosis despite symptom absence
Patient Communication
- Explaining why absence of pain does not necessarily indicate healing
- Addressing misconceptions(“no pain = no problem”)
Clinical Workflow Support
- Structuring symptom timelines across visits
- Highlighting clinically significant transitions
- Supporting consistent interpretation of symptom resolution
Emerging Direction
- Predictive models for pulp vitality and necrosis
- Integration of symptom history with diagnostic testing
- AI-assisted risk stratification
Clinical Relevance
The challenge is not diagnosing obvious necrosis — it is correctly interpreting symptom disappearance, identifying silent progression early, and intervening at the appropriate stage.
AI may eventually help:
- improve interpretation of symptom history,
- support timely intervention in ambiguous presentations,
- reduce delayed treatment caused by false reassurance,
- and enhance patient communication clarity.
References
- European Society of Endodontology (ESE). Quality Guidelines for Endodontic Treatment. International Endodontic Journal. 2023.
- American Association of Endodontists (AAE). Endodontic Diagnosis. AAE Clinical Resources.
- Ricucci D, Siqueira JF Jr, Rôças IN. Pulp Response to Periodontal Disease: Novel Observations Help Clarify the Processes of Tissue Breakdown and Infection. J Endod.
- Seltzer S, Bender IB, Ziontz M. The dynamics of pulp inflammation: correlations between diagnostic data and actual histologic findings. Oral Surgery, Oral Medicine, Oral Pathology.
- Hargreaves KM, Berman LH. Cohen’s Pathways of the Pulp. Elsevier.
- Lin LM, Ricucci D, Saoud TM, Sigurdsson A, Kahler B. Vital pulp therapy of mature permanent teeth with irreversible pulpitis from the perspective of pulp biology. Australian Endodontic Journal.
- Jafarzadeh H, Rosenberg PA. Pulse oximetry: review of a potential aid in endodontic diagnosis. Journal of Endodontics.
- The Use of Artificial Intelligence in Endodontics - F.C. Setzer, J. Li, A.A. Khan, 2024